Is your case great enough to be selected for our Wall of Fame? If so, we’ll post your name and case here for the world to see!
10/23: Evgenii Chernov
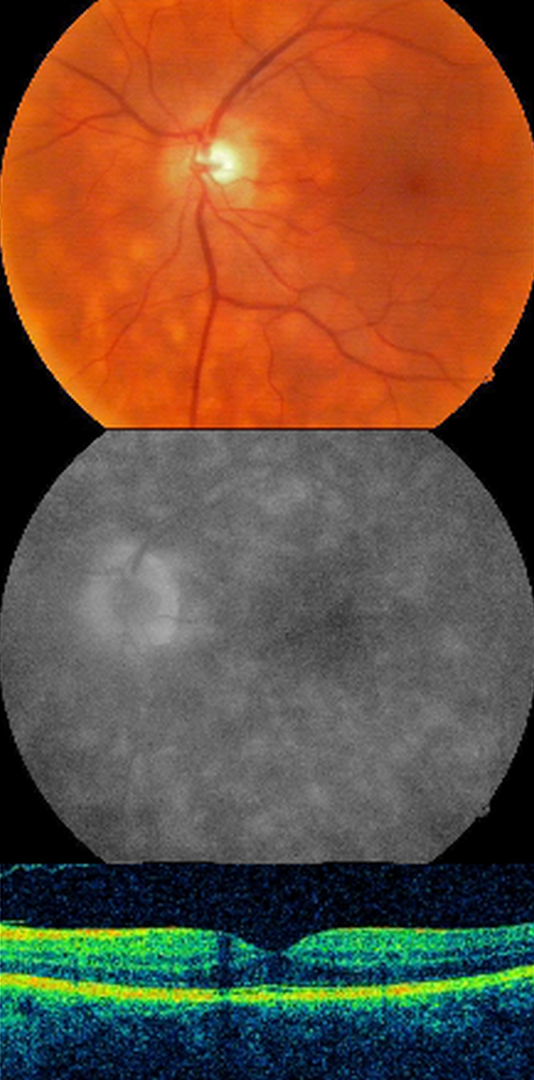
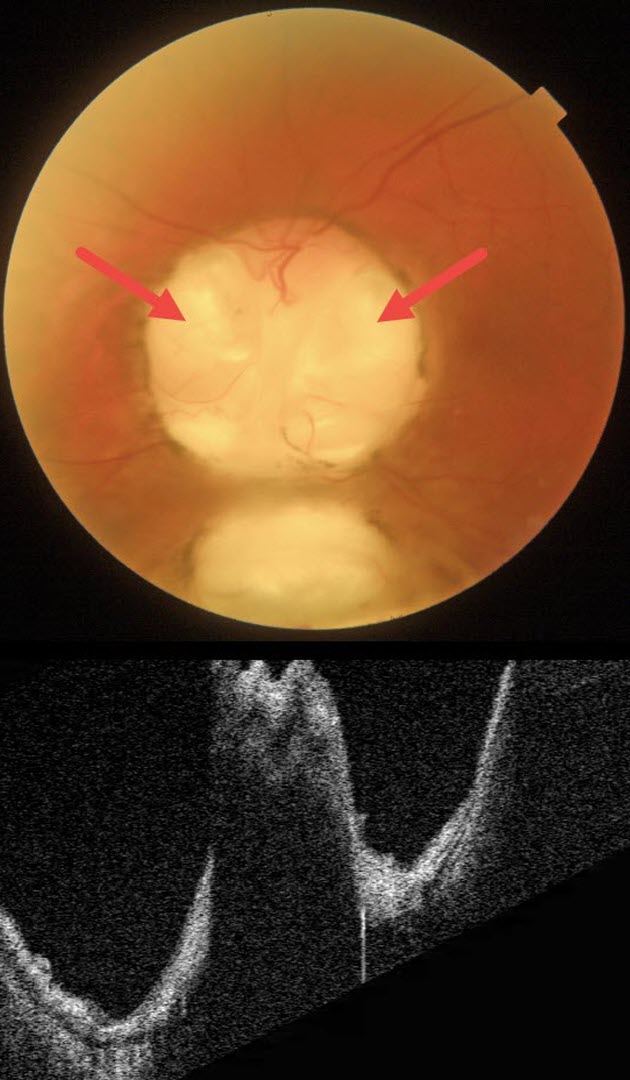
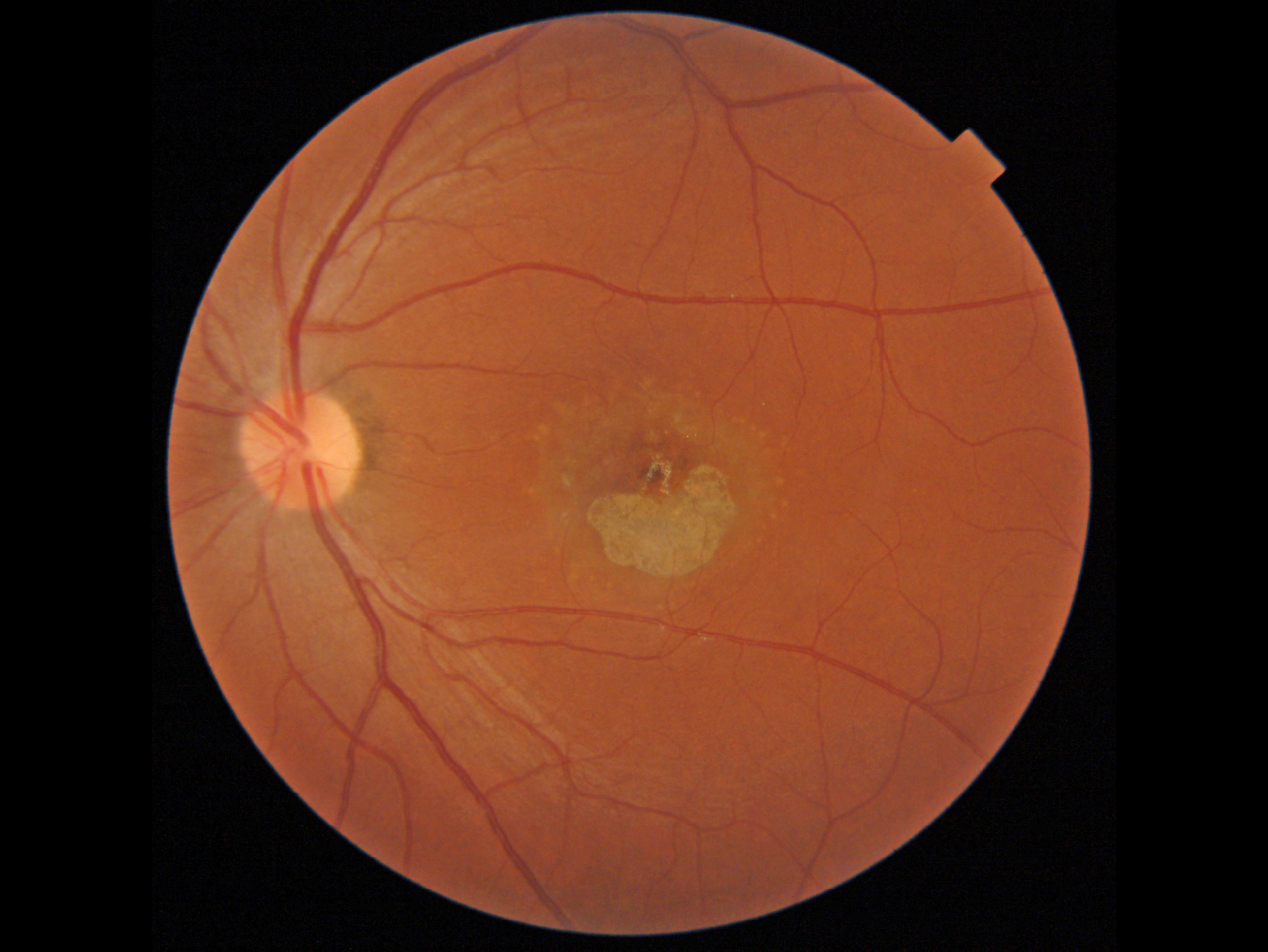
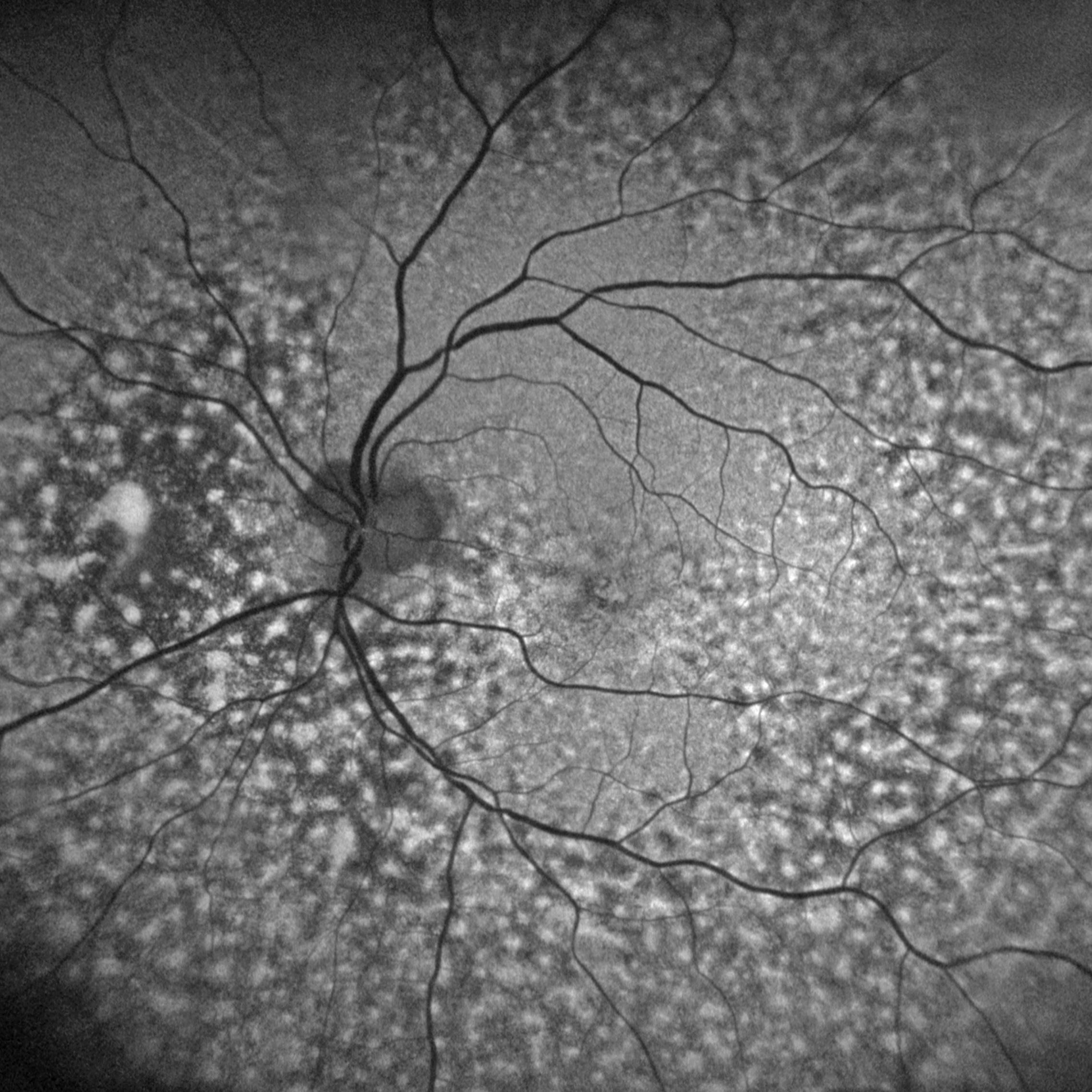
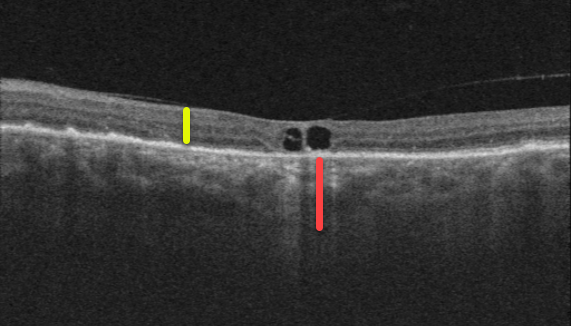
Best Disease
9/24: Anjana Mirajkar and Manish Nagpal
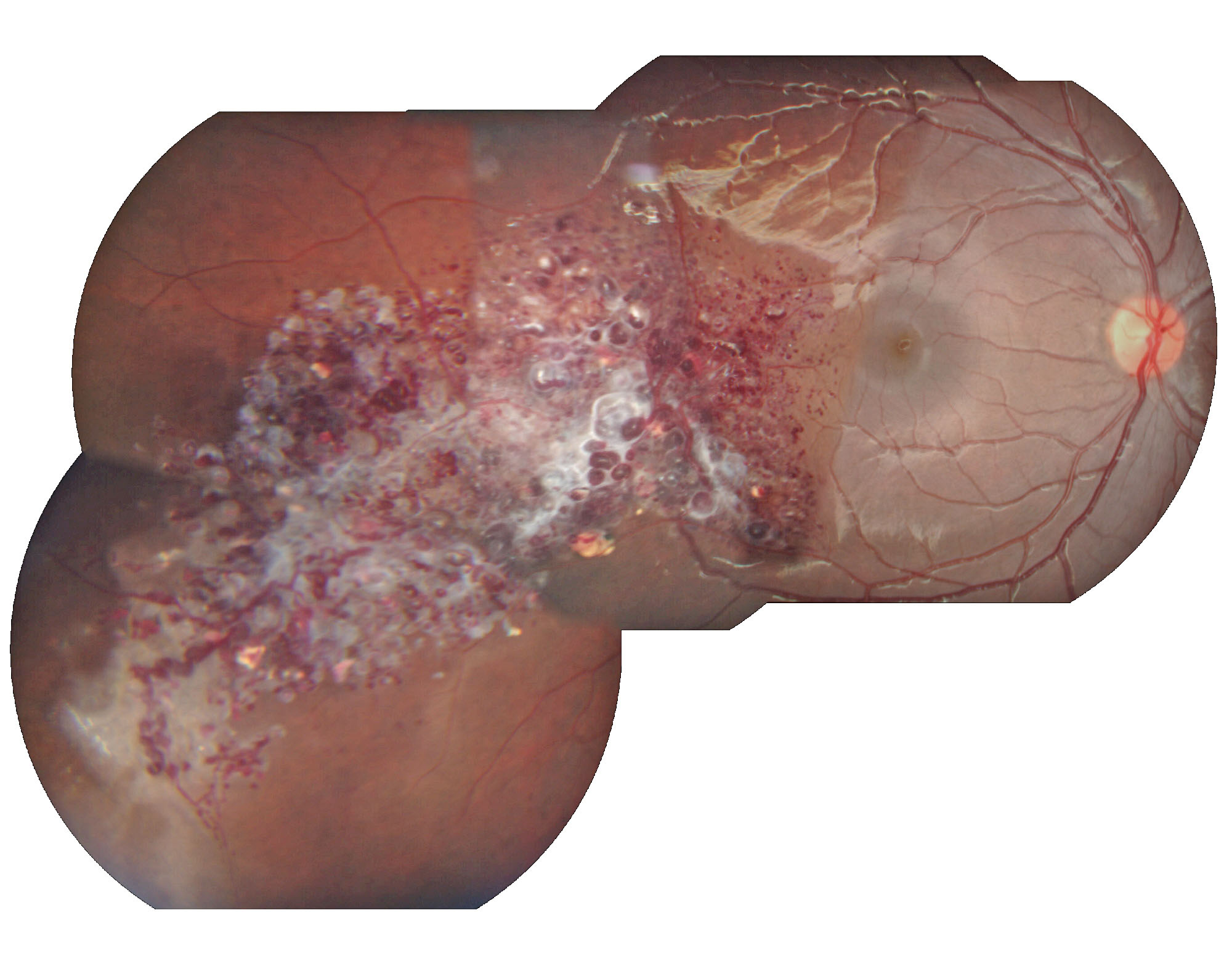
Intraocular Foreign Body
8/24: Anjana Mirajkar and Manish Nagpal
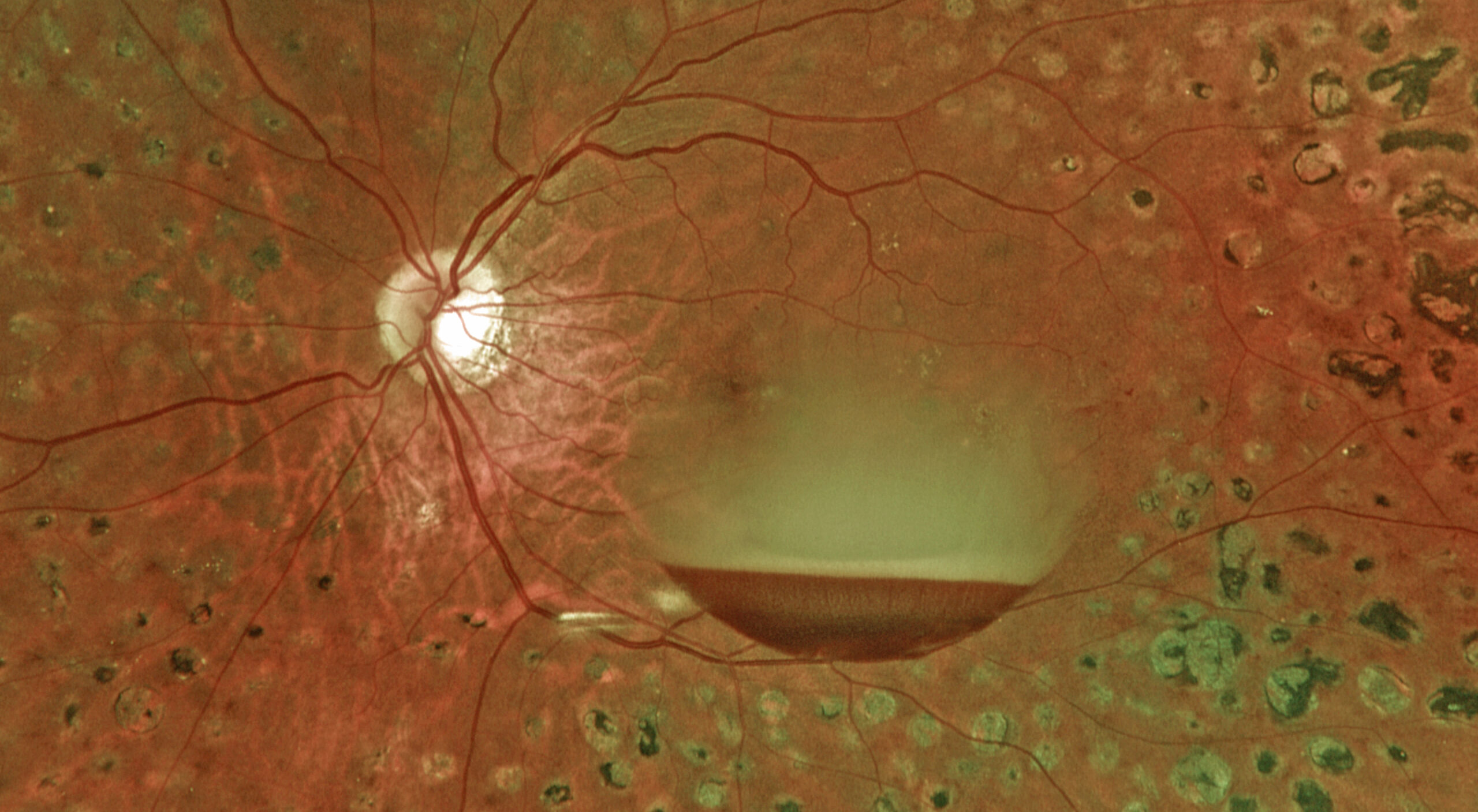
Pseudopapilledema from leukemic optic nerve infiltration
7/24: Justin Grassmeyer, Ambar Faridi, and Brittany Heckerman
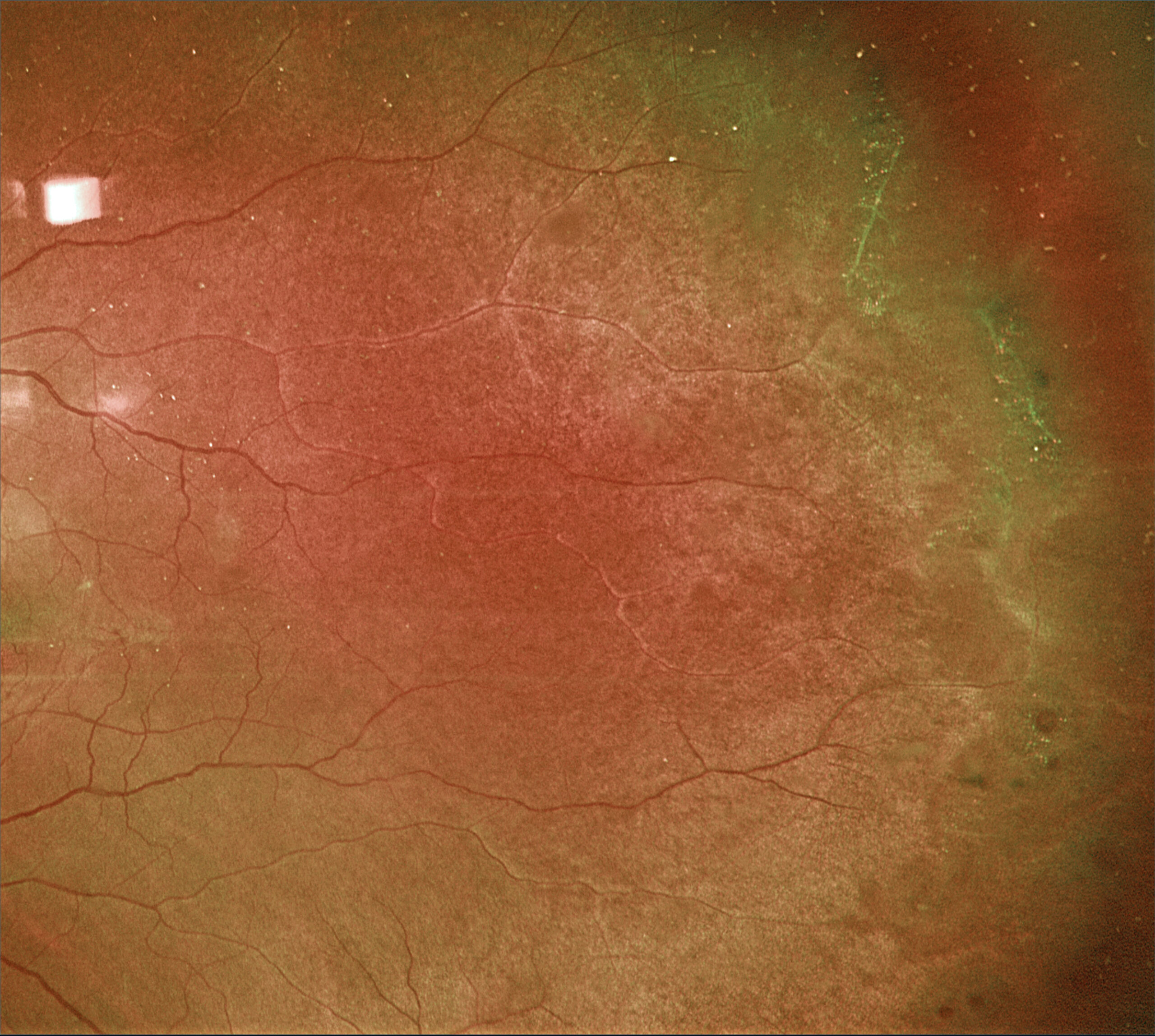
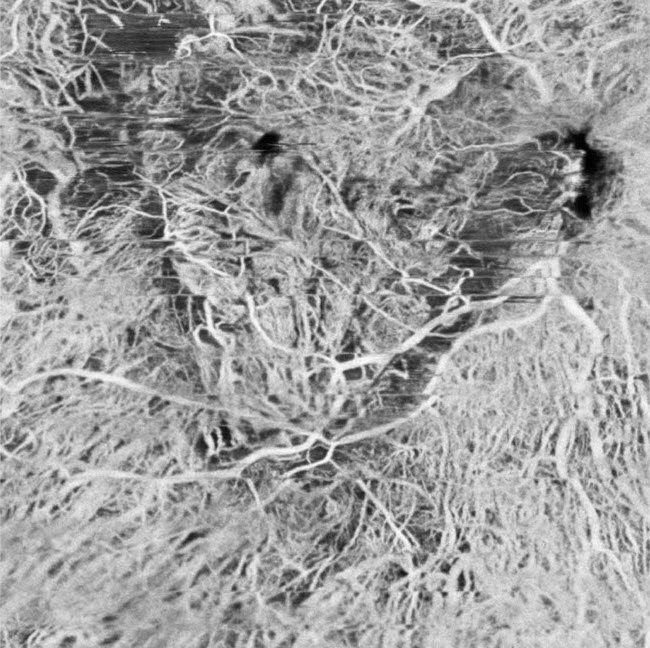
Lattice degeneration
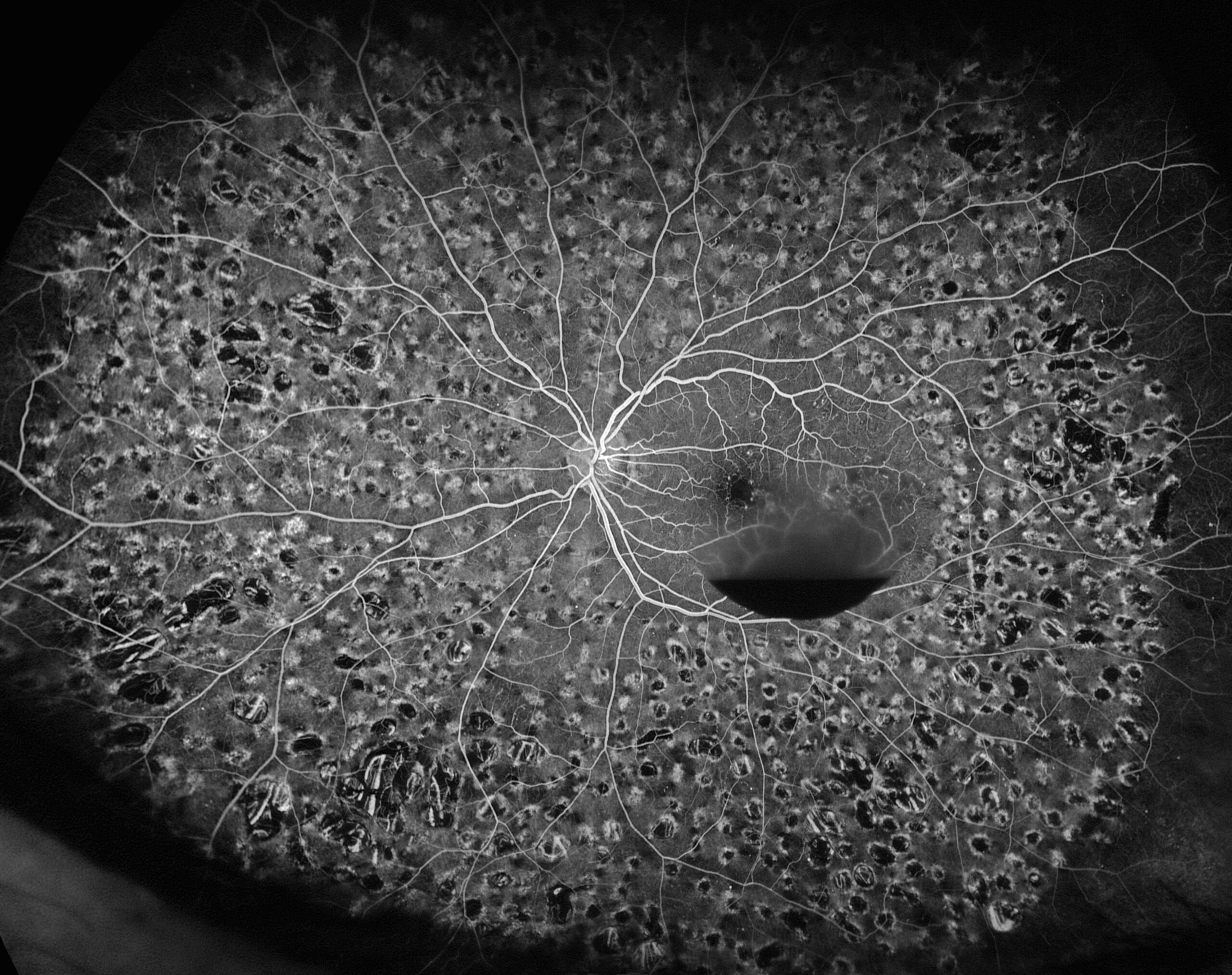
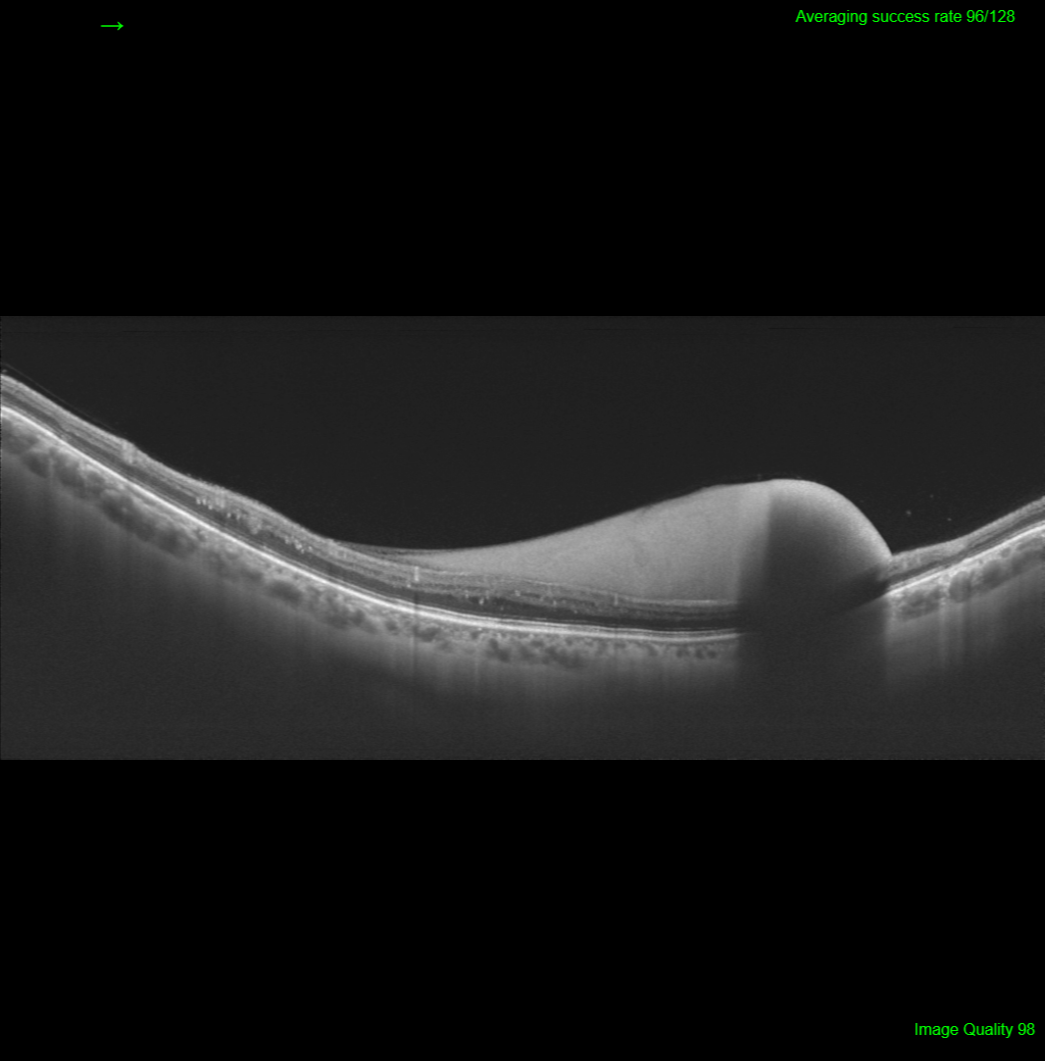
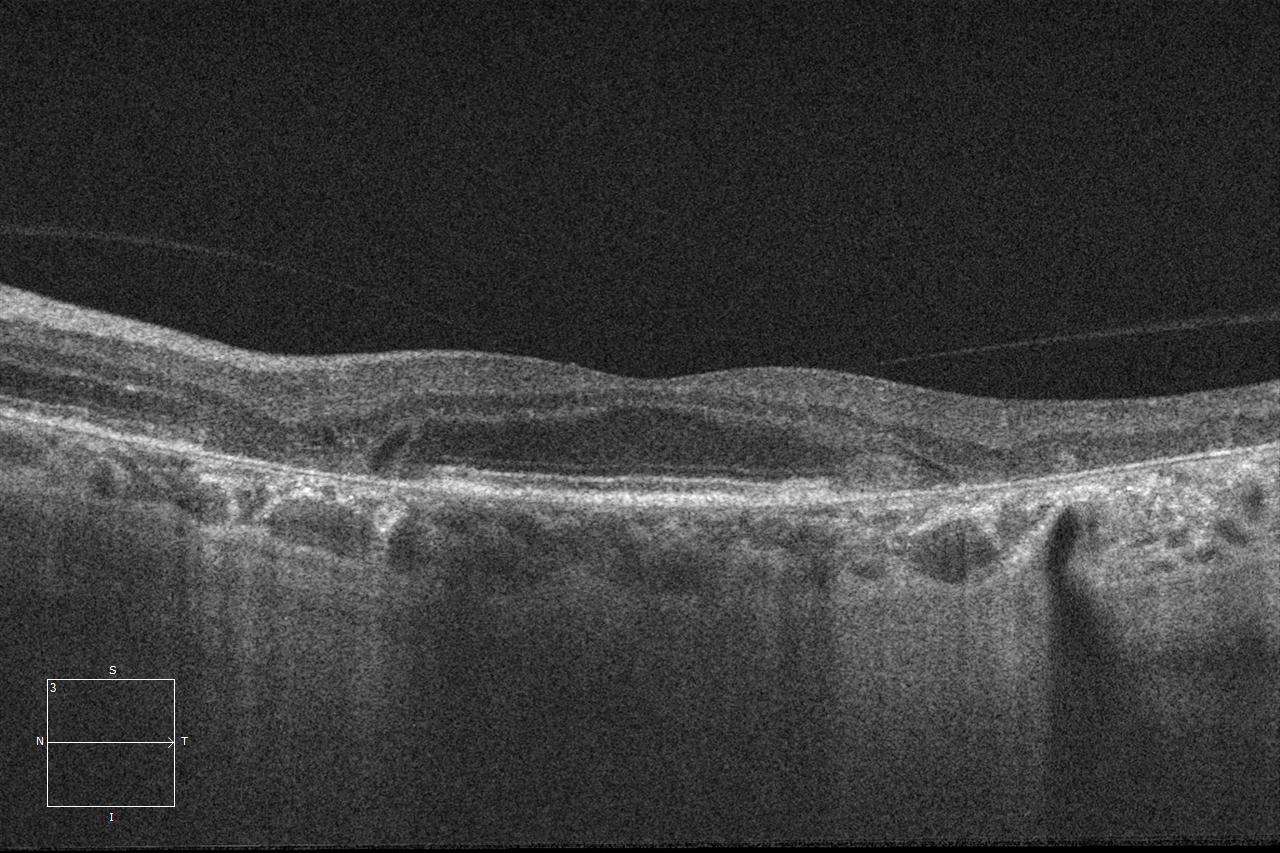
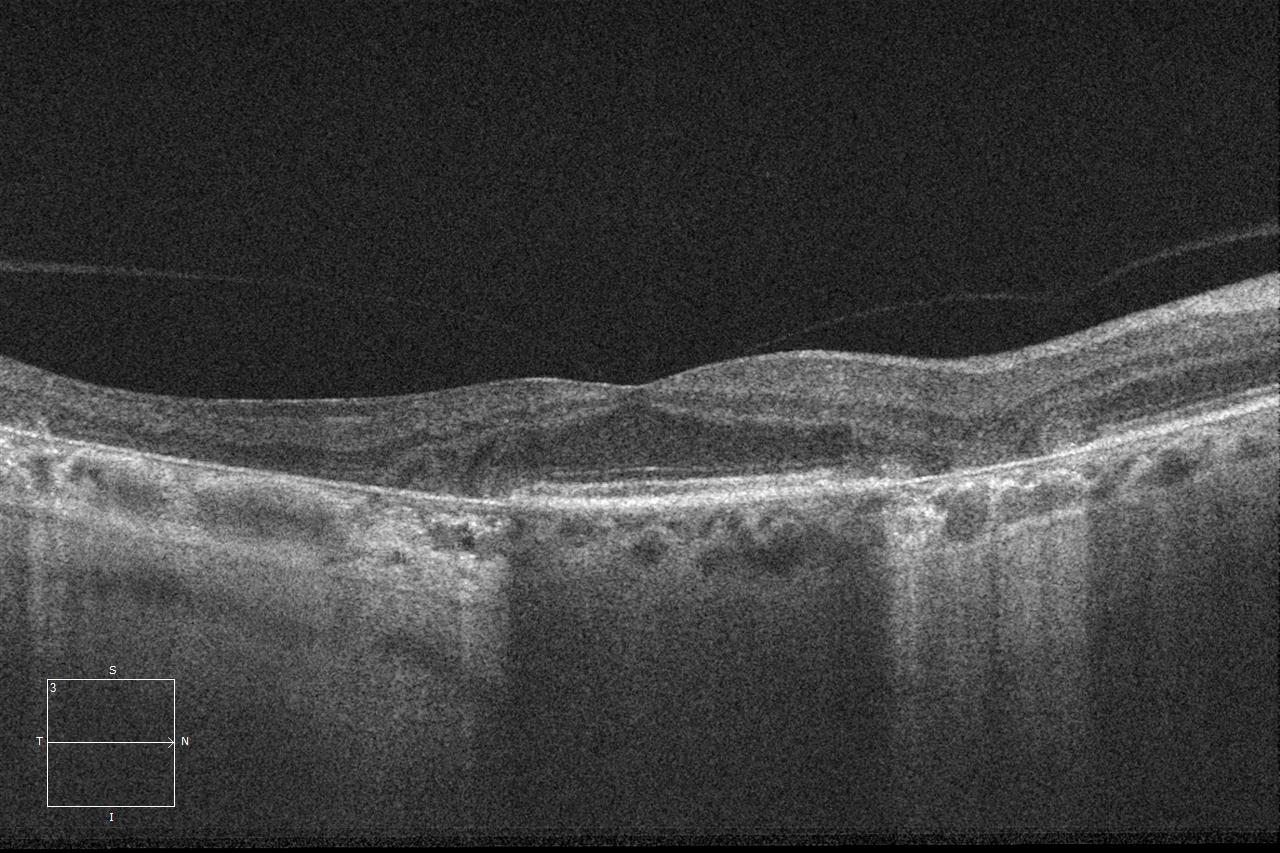
6/24: Ogugua Okonkwo, Adekunle Olubola Hassan, Ayodele Harriman, Ogochukwu Sibeudu, and Idris Akintayo Oyekunle
Tuberculous serpiginous-like choroiditis
5/24: Seif Anwar
Inherited Retinal Disease
Sengül Özdek and Ece Özdemir Zeydanlı
Case of the Year winner!
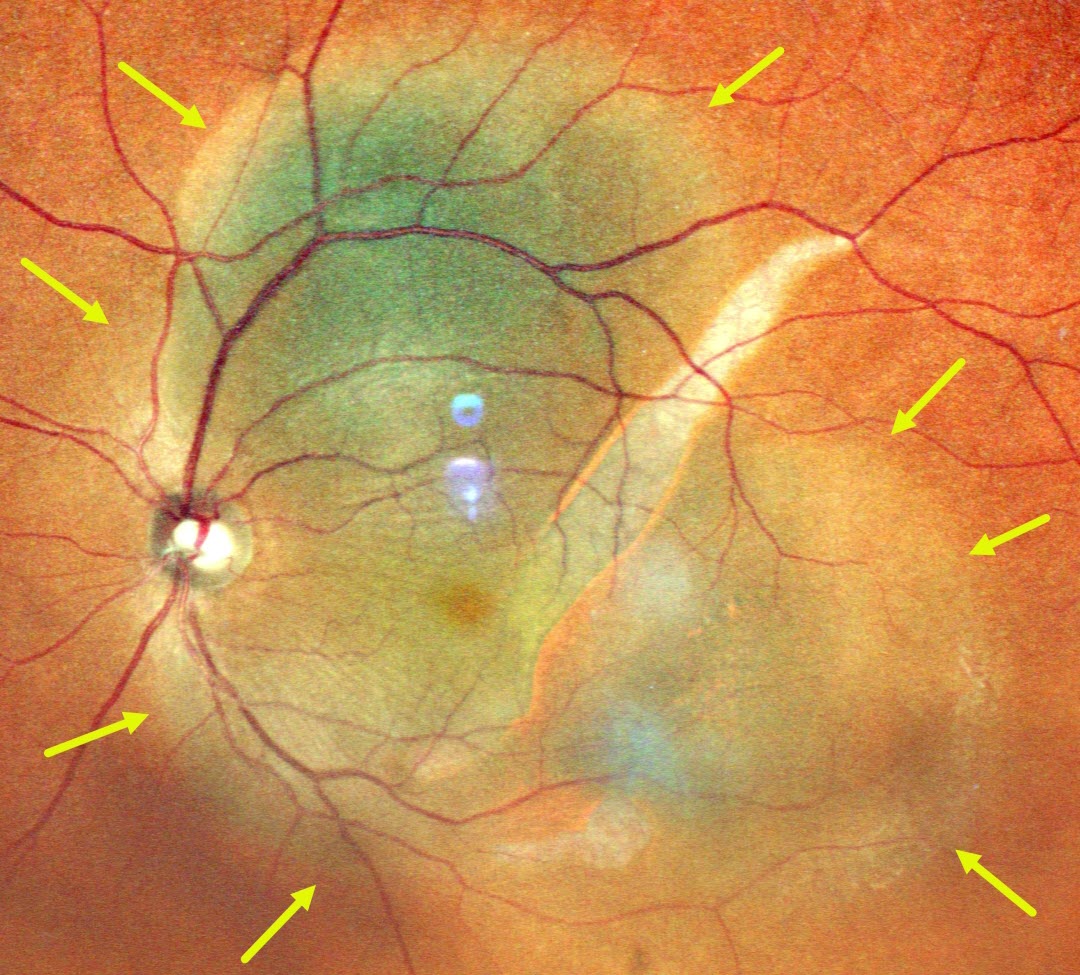
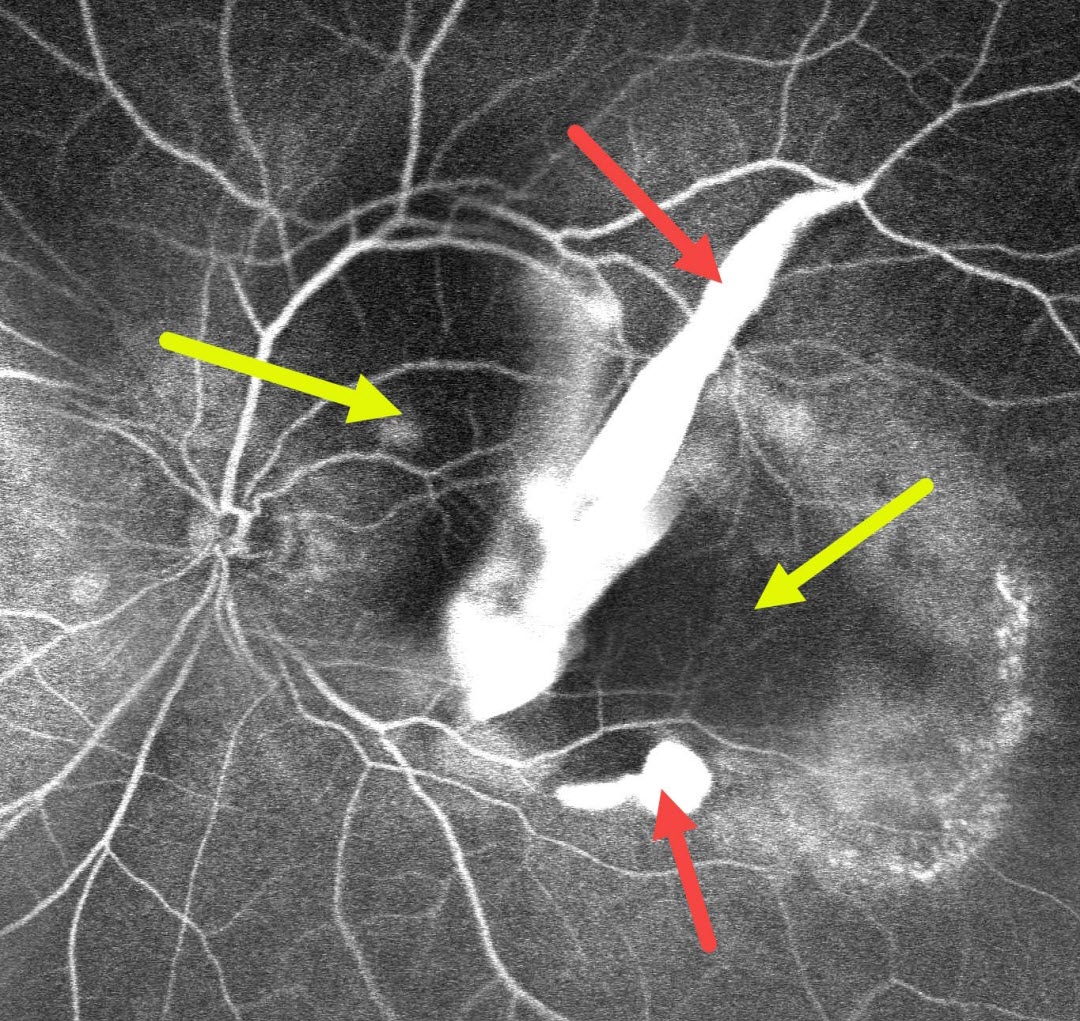
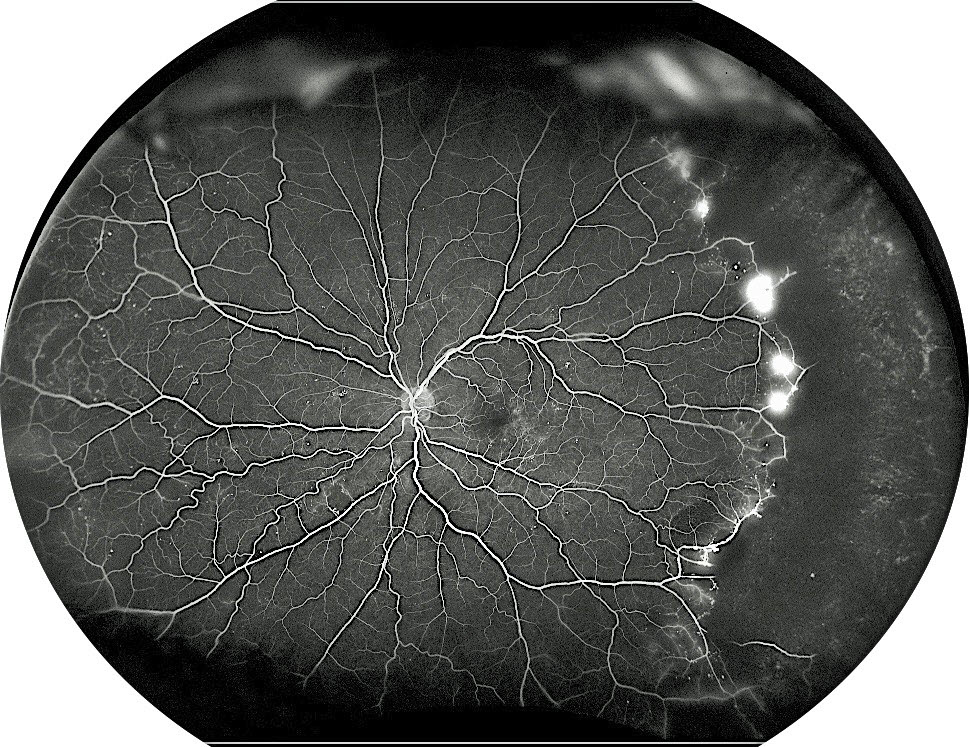
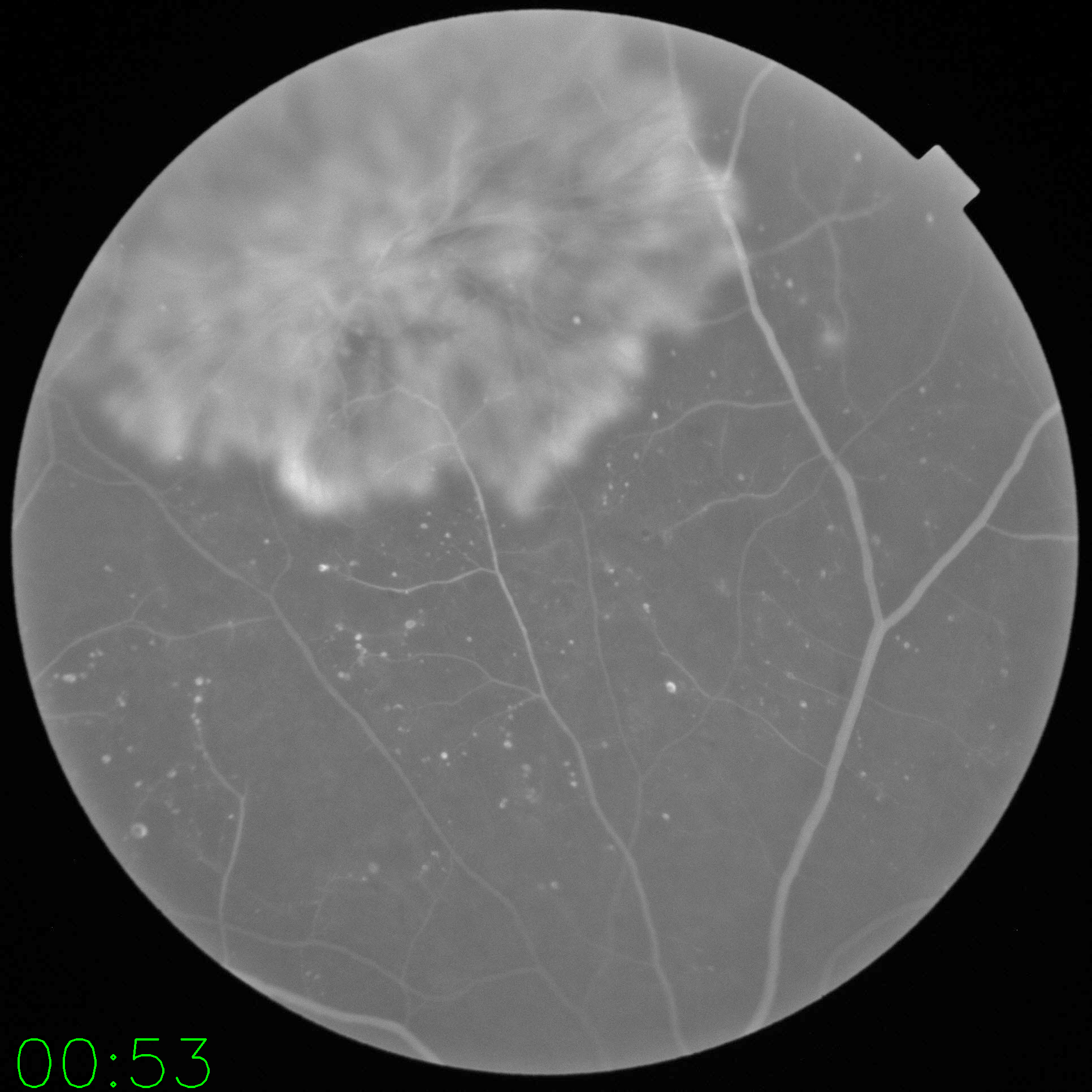
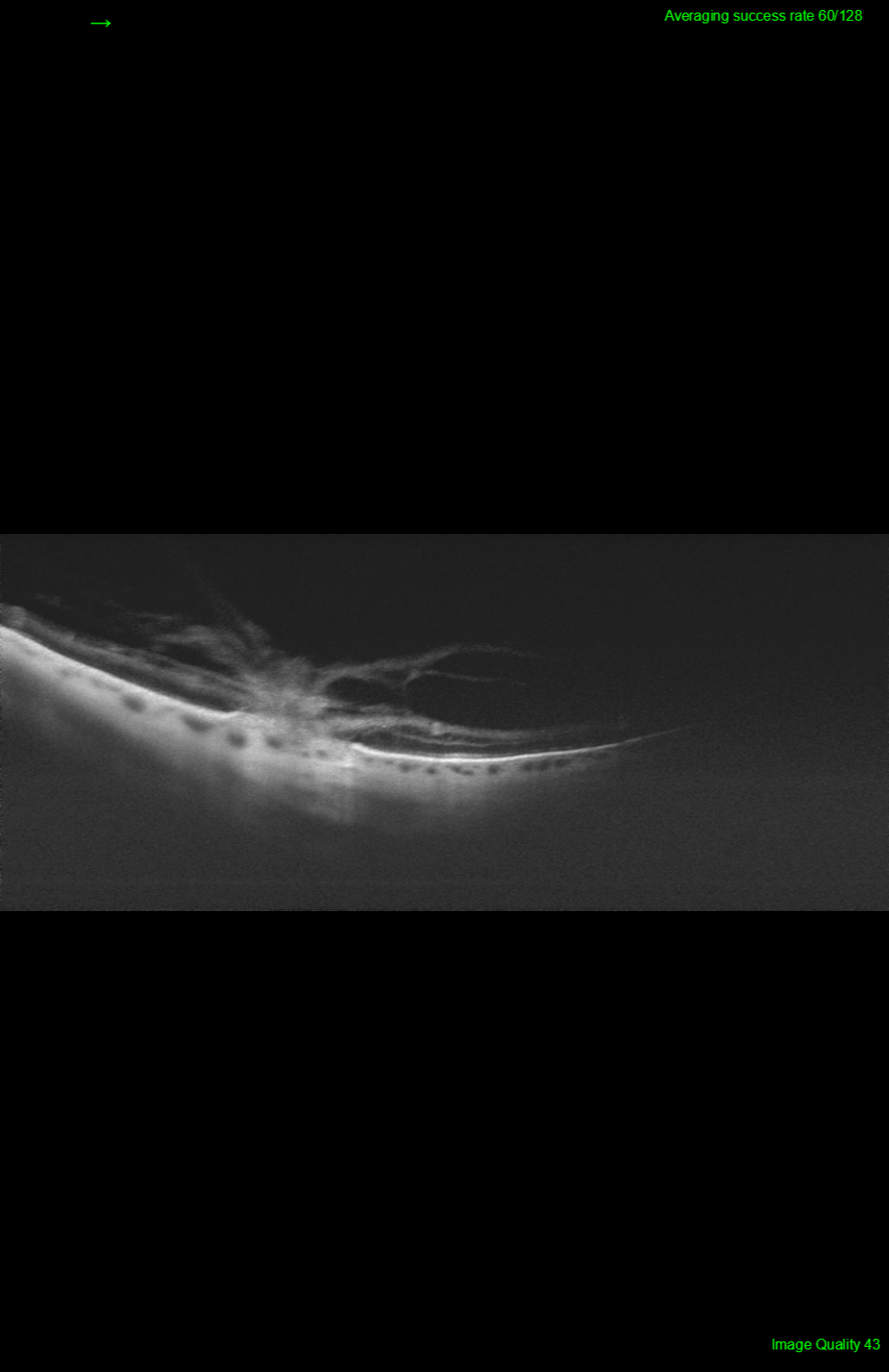
Retinal Arteriovenous Malformation
4/24: Kanwaljeet Harjot Madan
Shaken baby syndrome
3/24: Ayushi Gupta and Vishal Agrawal
Benign familial fleck retina
2/24: Will Gibson
Retinal venous malformation
12/23: Anjana Mirajkar and Manish Nagpal
Central retinal artery occlusion with cilioretinal sparing
11/23: Anjana Mirajkar and Manish Nagpal
Harada’s Disease
10/23: Will Gibson
Posterior scleritis with chorioretinal folds
9/23: Shivraj Tagare and Nishant Maindargi
Valsalva retinopathy drained with YAG laser
8/23: Mohammad Abbas
Laser-induced retinal break and vitreous hemorrhage
7/23: Joe Yuenpang Cheung
Group-type congenital pigmented nevi of the RPE (bear tracks)
6/23: Gil Calvão-Santos and Keissy Sousa
Waardenburg Syndrome
5/23: Natasa Draca and Ratko Lazic
Tattoo-induced Uveitis
4/23: Veronika Matello and Barbara Parolini
Case of the Year winner!
The EmPuzzled Eye
3/23: Emma Oreskovic and Natasha Draca
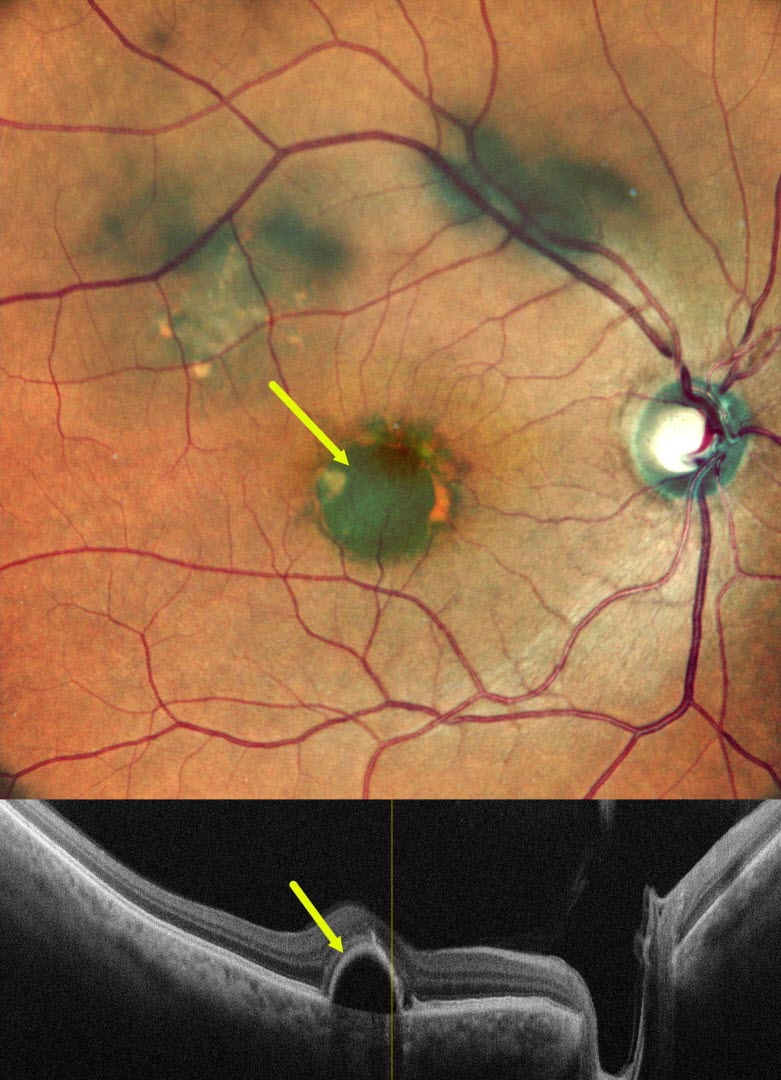
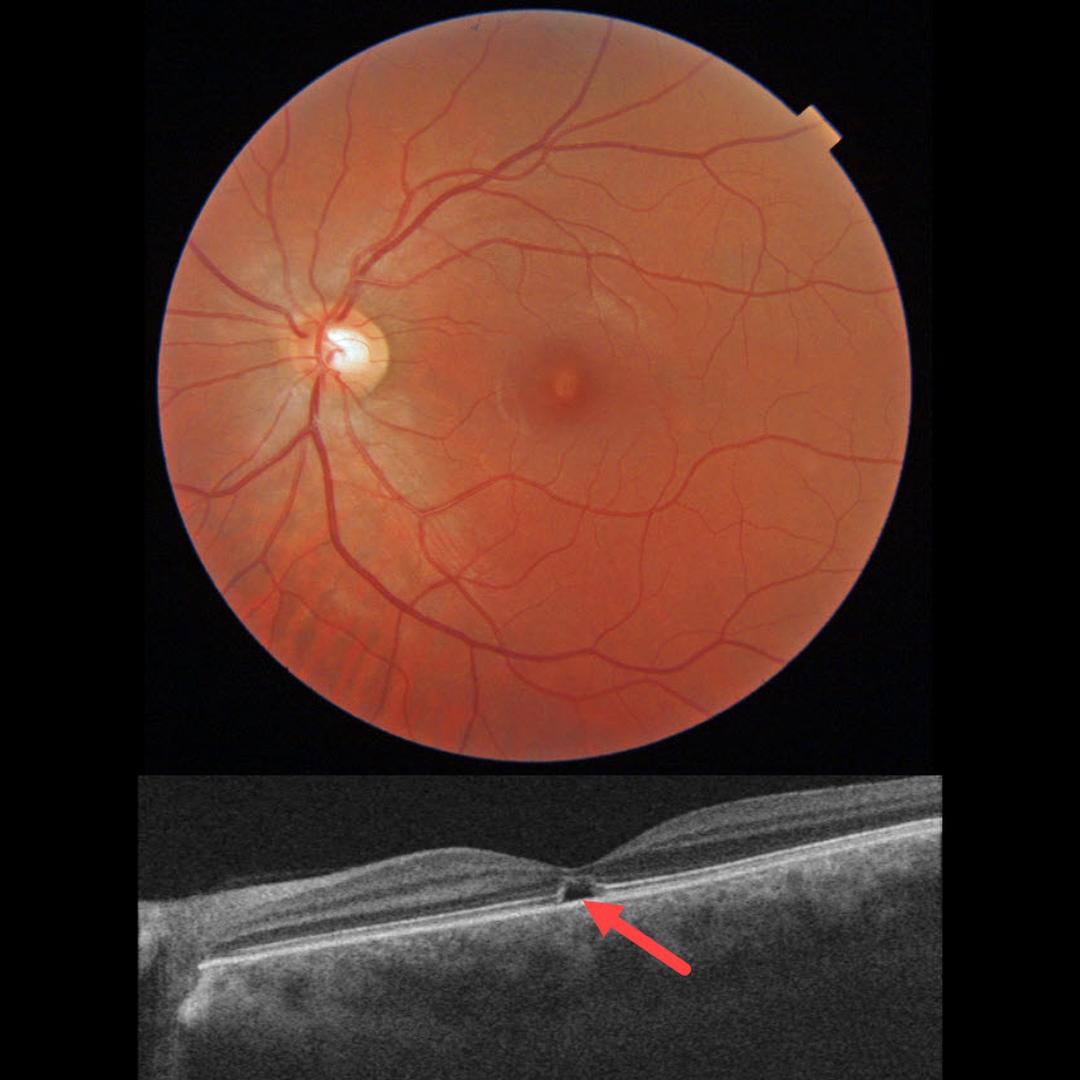
Optic Nerve Pit
2/23: Anjana Mirajkar
Giant RPE Tear
11/22: Veronika Matello and Barbara Parolini
Choroidal Hemangioma Widefield OCT
8/22: Nivesh Gupta
Ischemic Central Retinal Vein Occlusion
7/22: Omar Mulki:
Choroidal Osteoma
3/22: Erdem Dinç
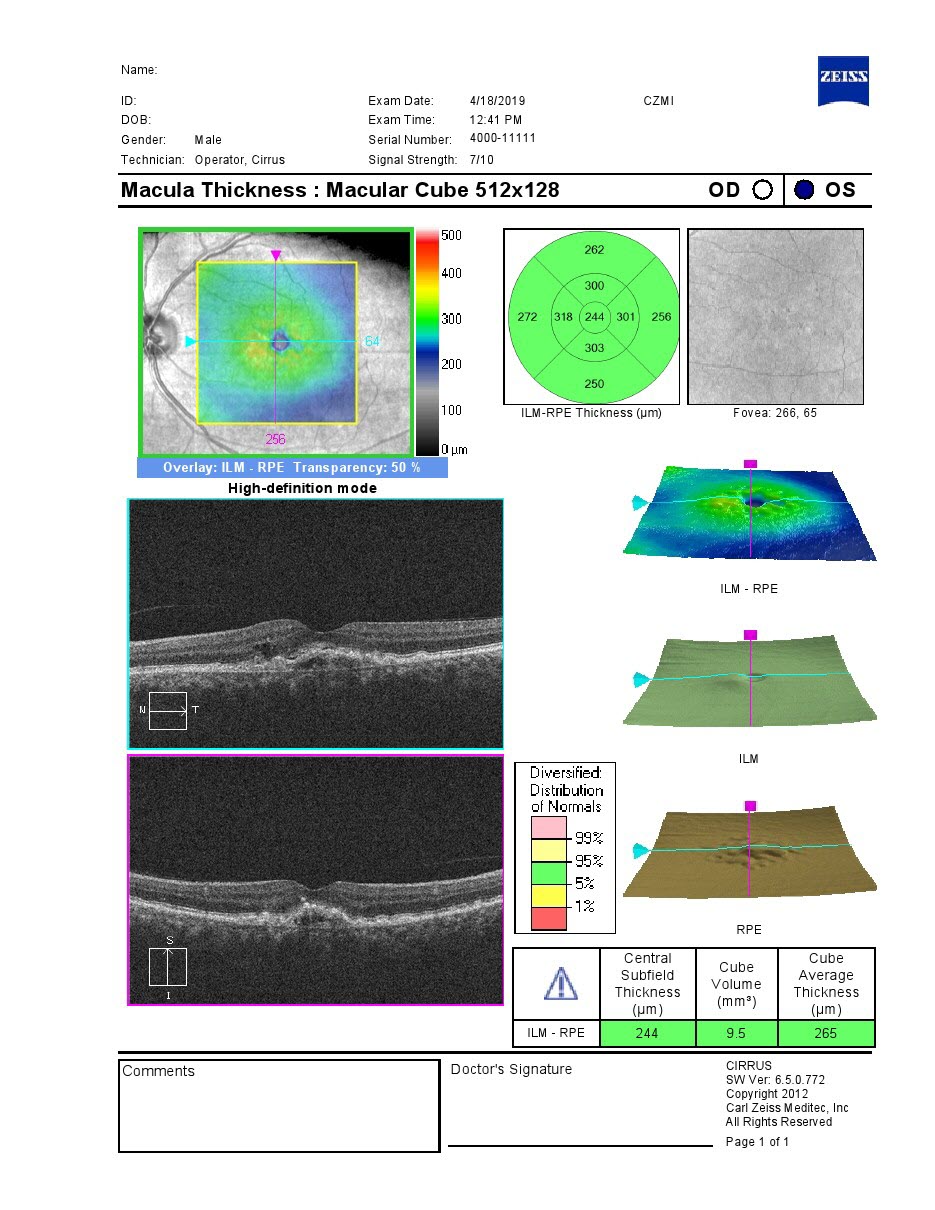
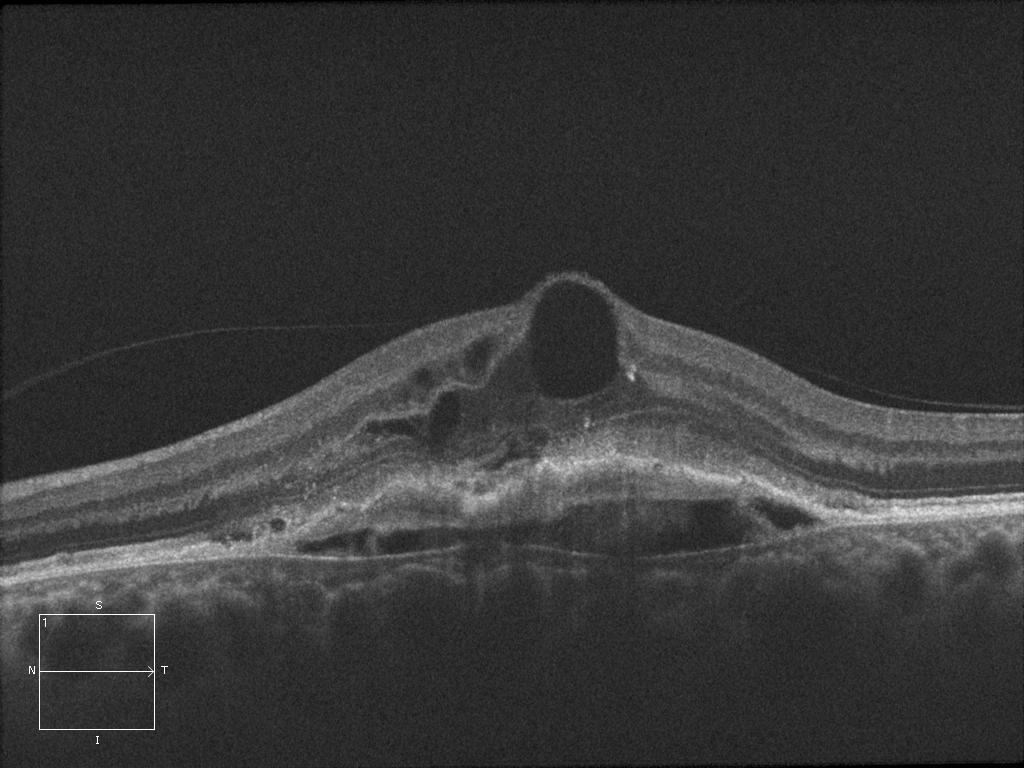
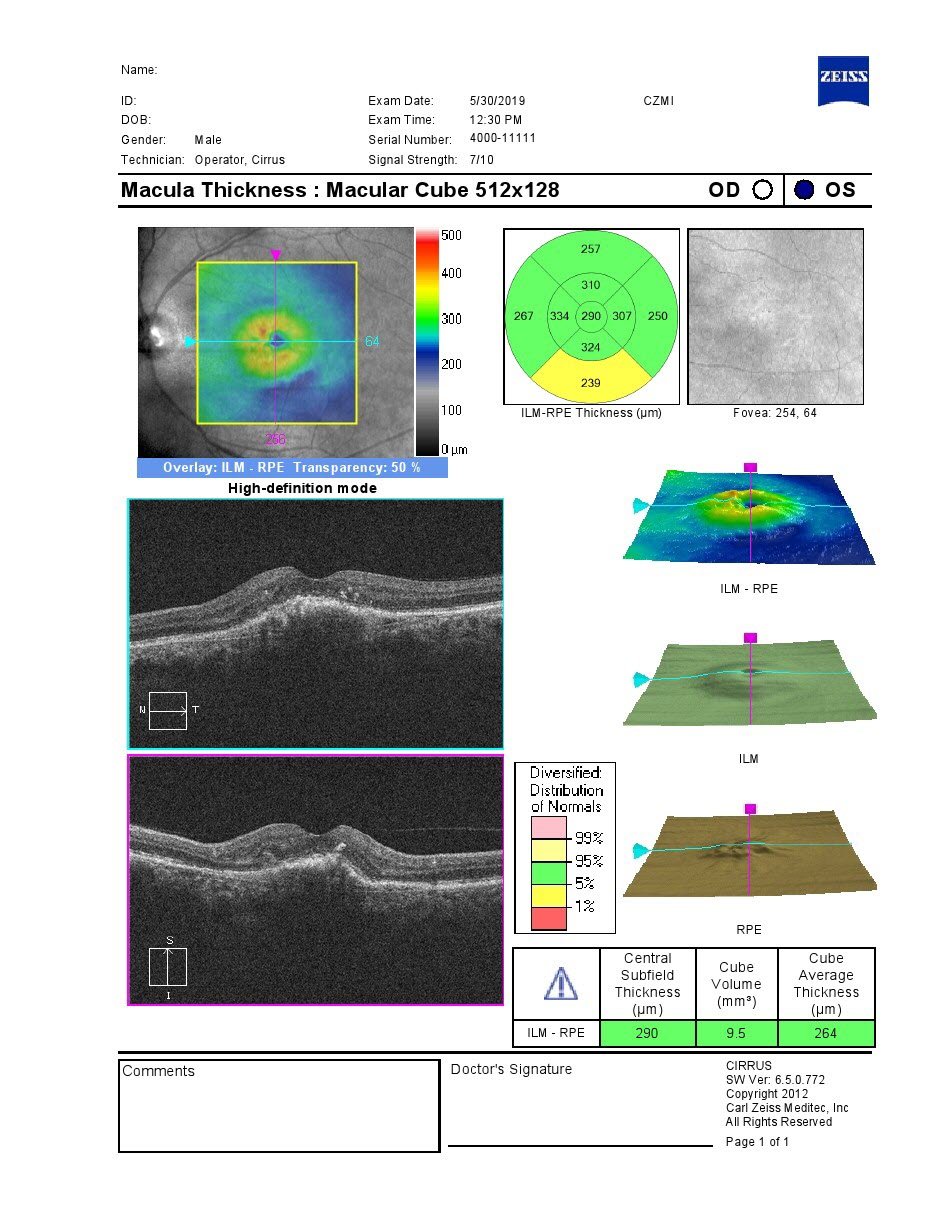
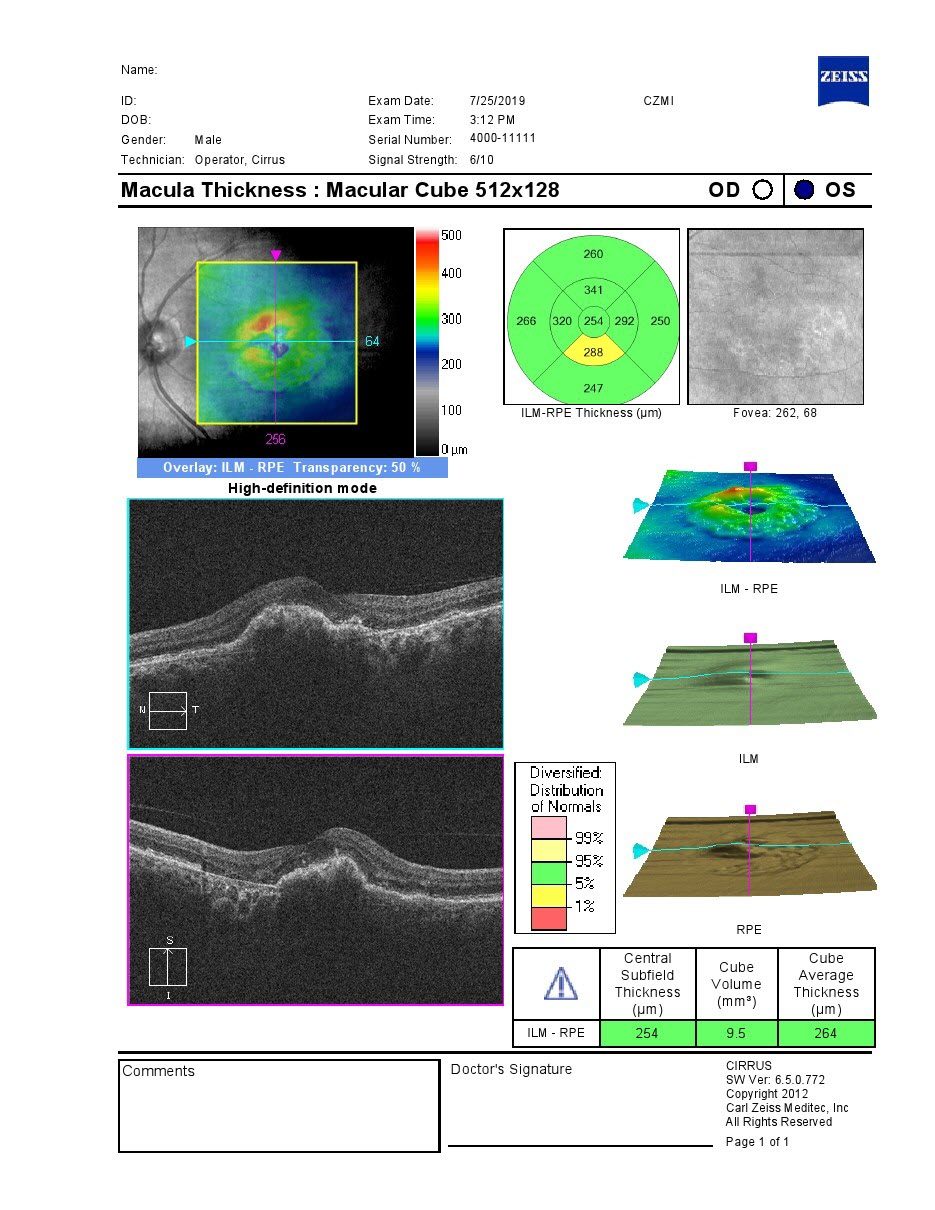
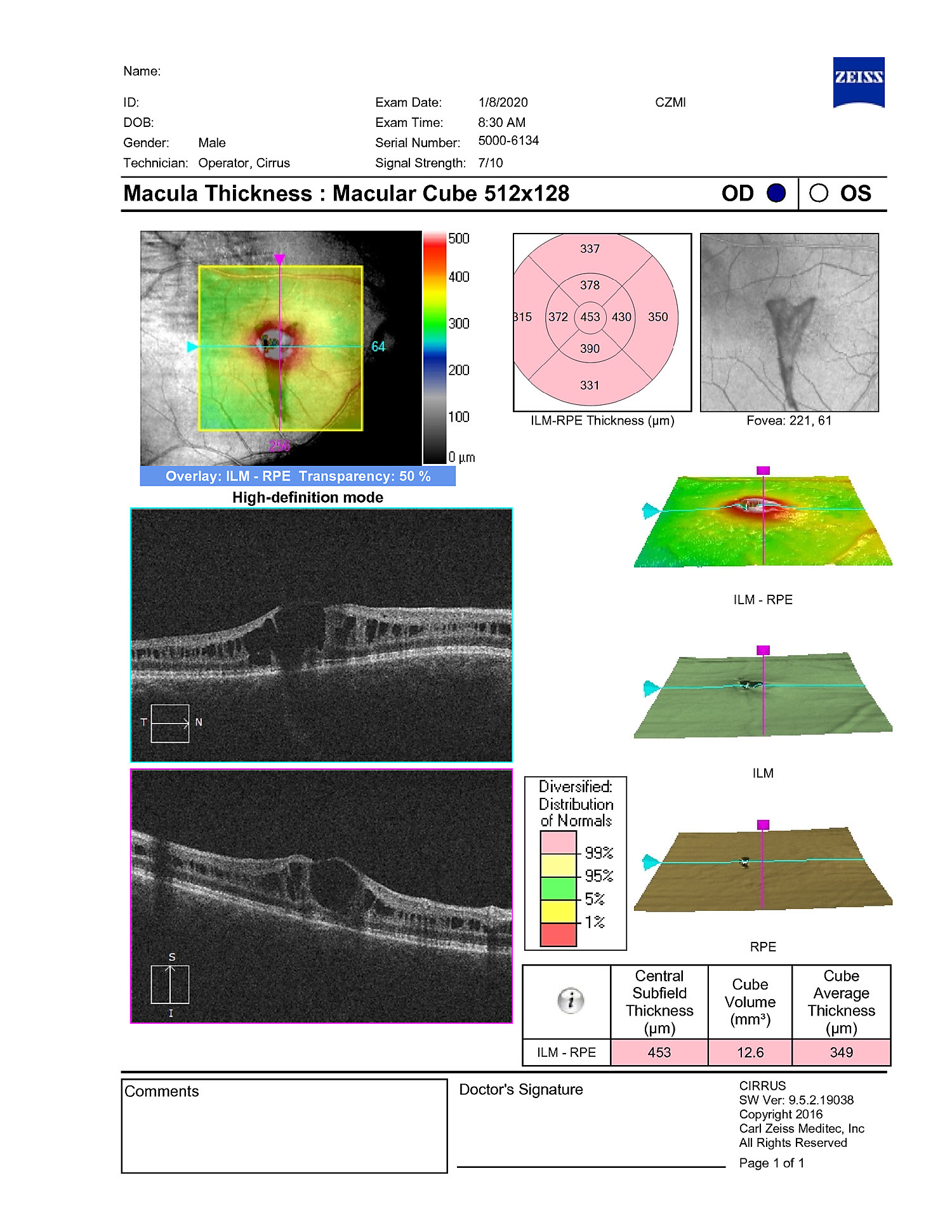
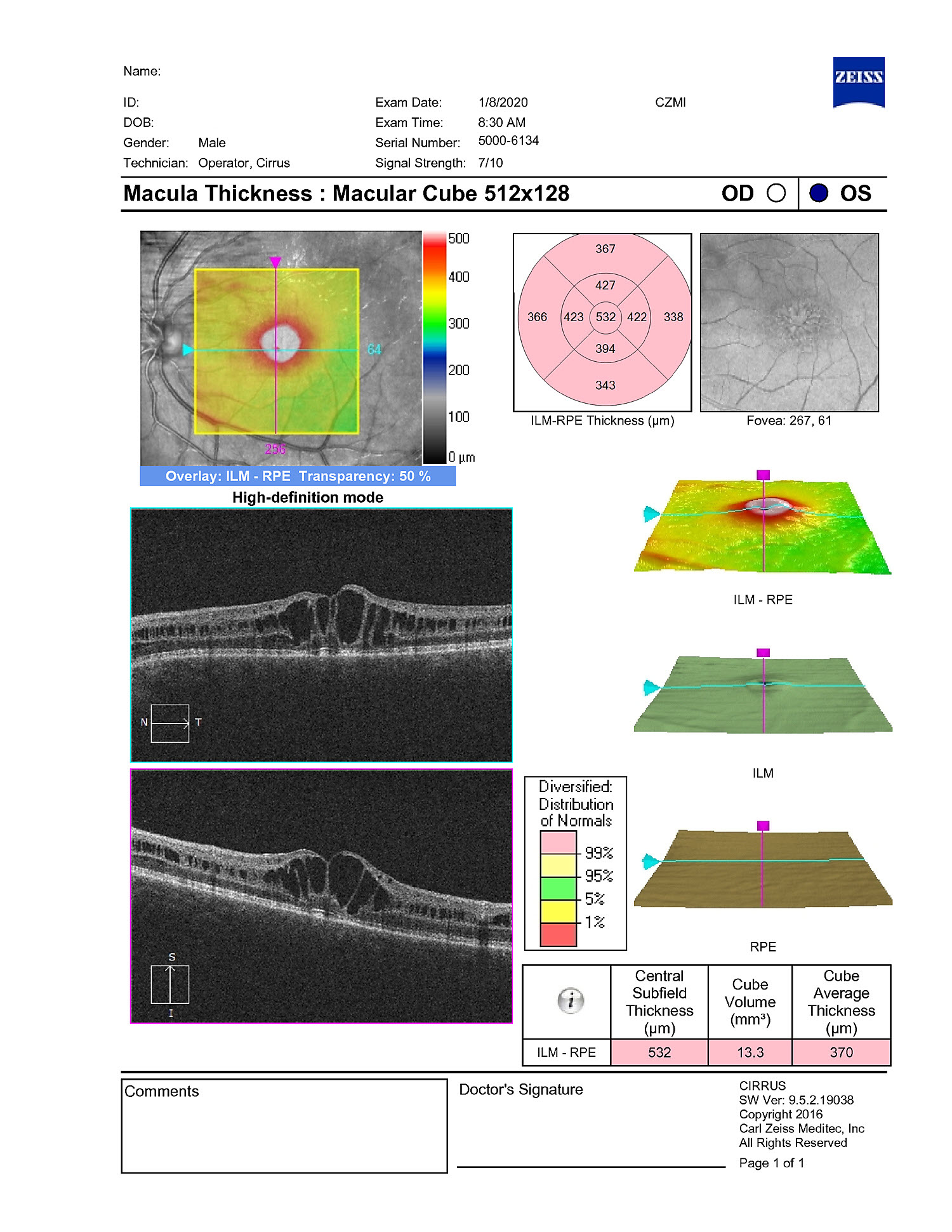
Is Temporary ILM Flap Sufficient for MH Closure?
1/22: Veronika Matello and Barbara Parolini
Case of the Year winner!
Choroidal Transplant for Subfoveal AMD MNV
12/21: Otis Hertsenberg
Optic Nerve Coloboma with Pit
11/21: David Kilpatrick
Frosted Branch Angiitis from Sarcoidosis
10/21: Kumar Chugani
Coats Disease
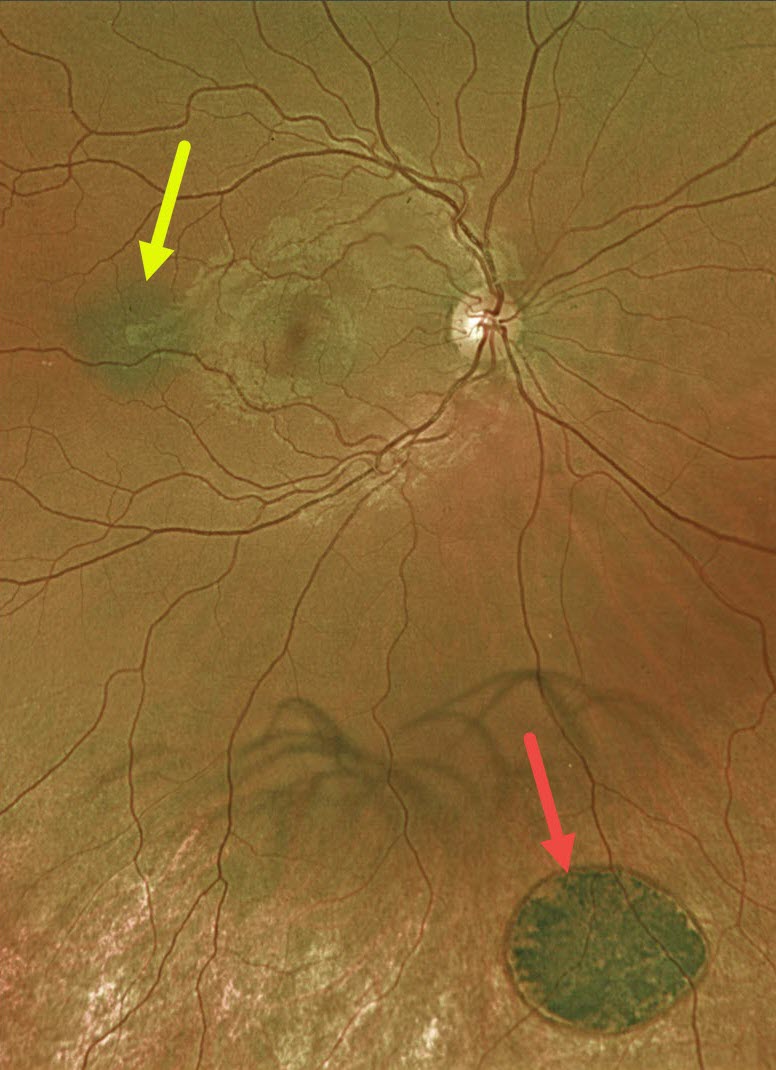
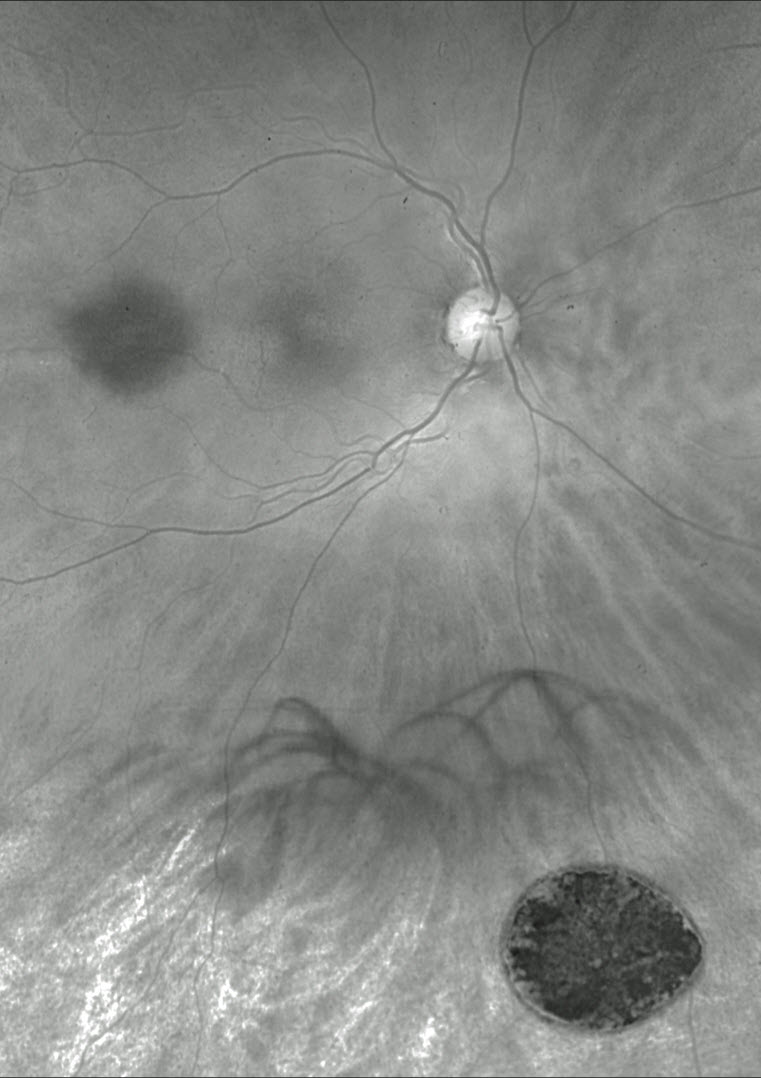
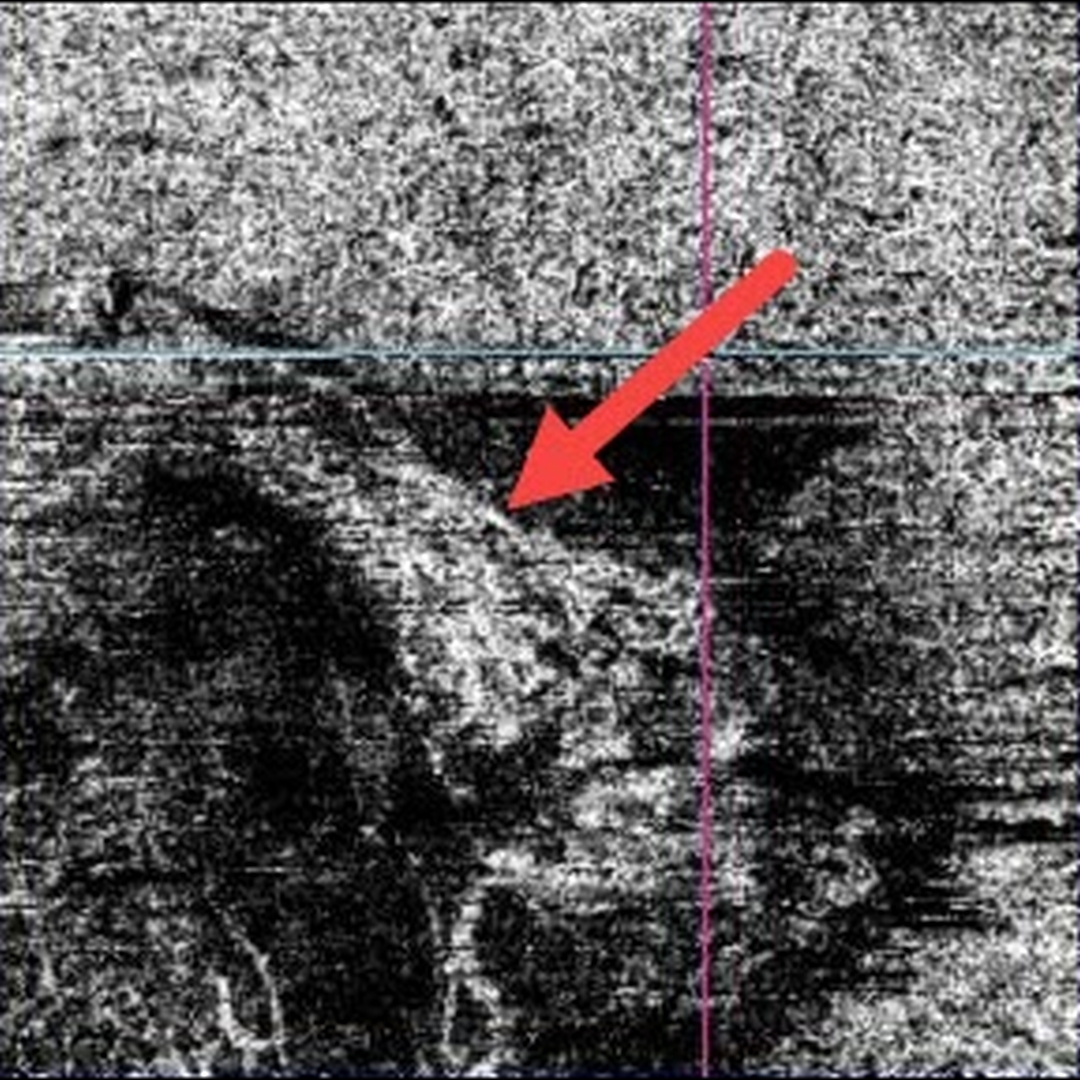
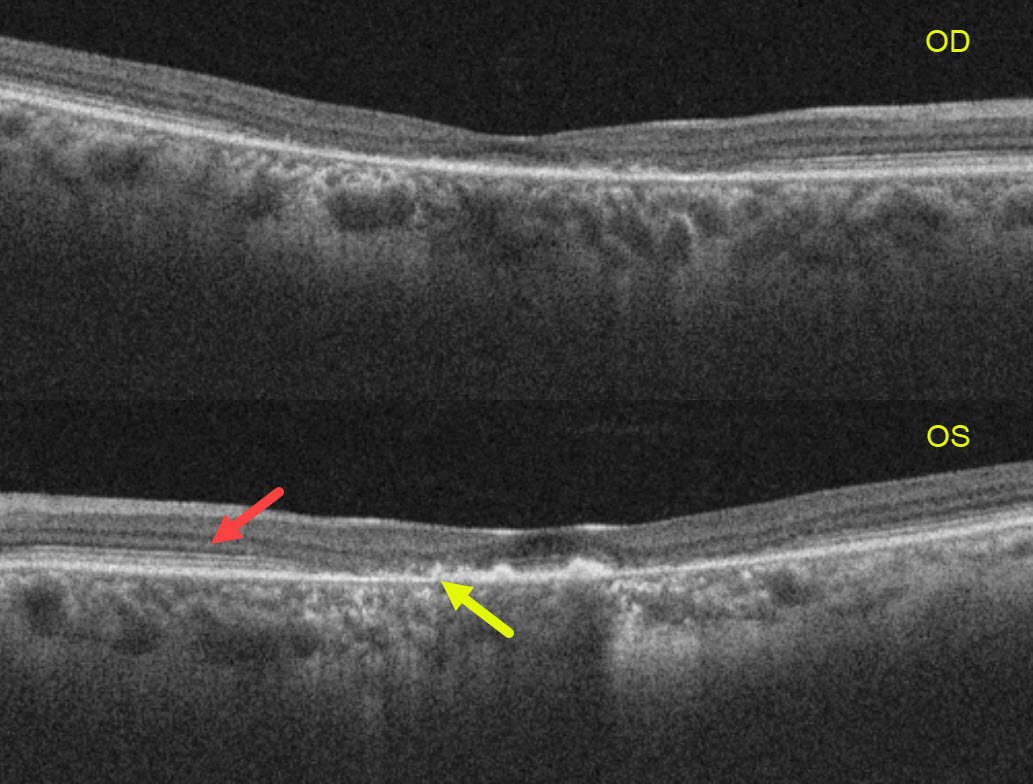
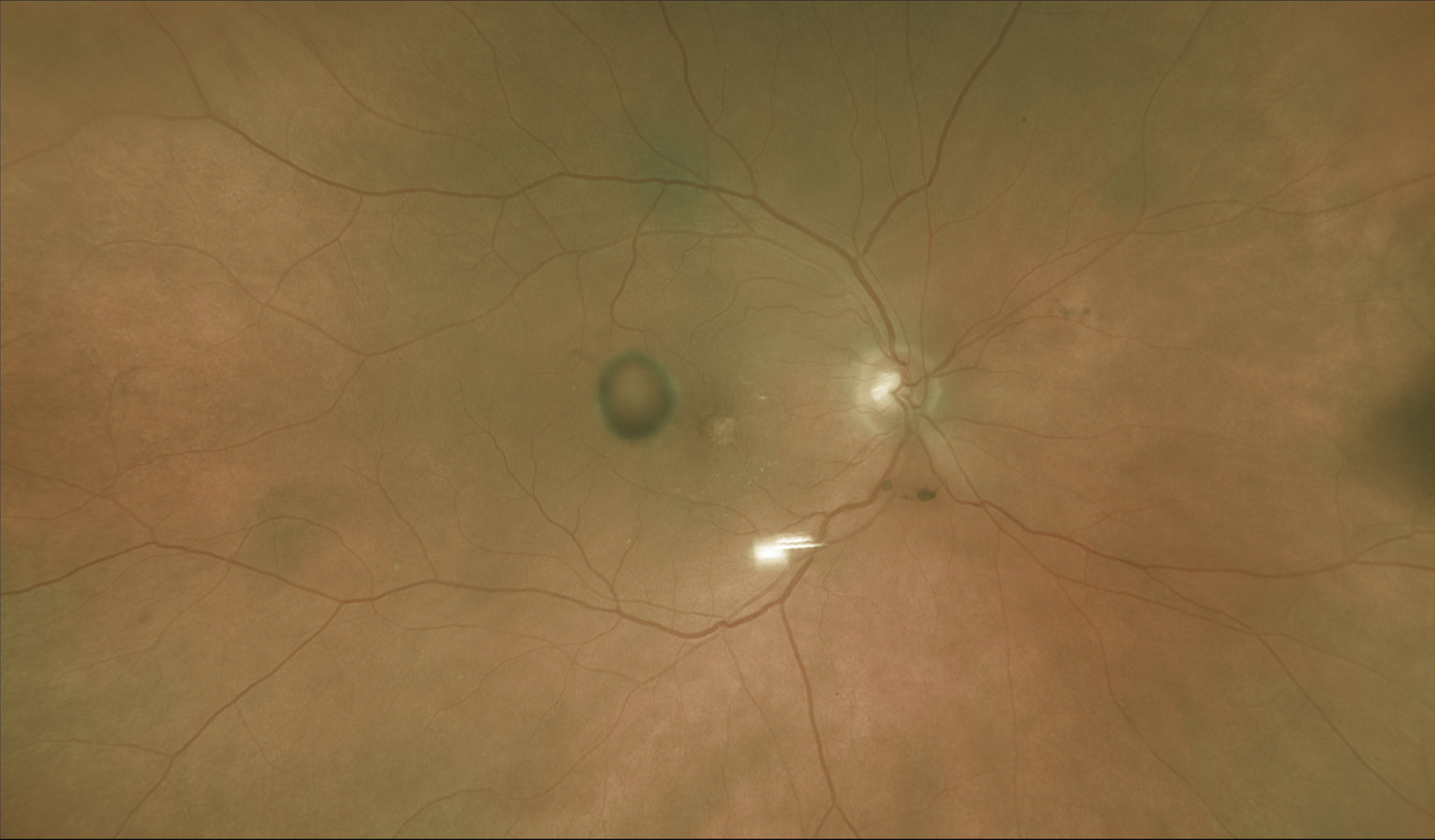
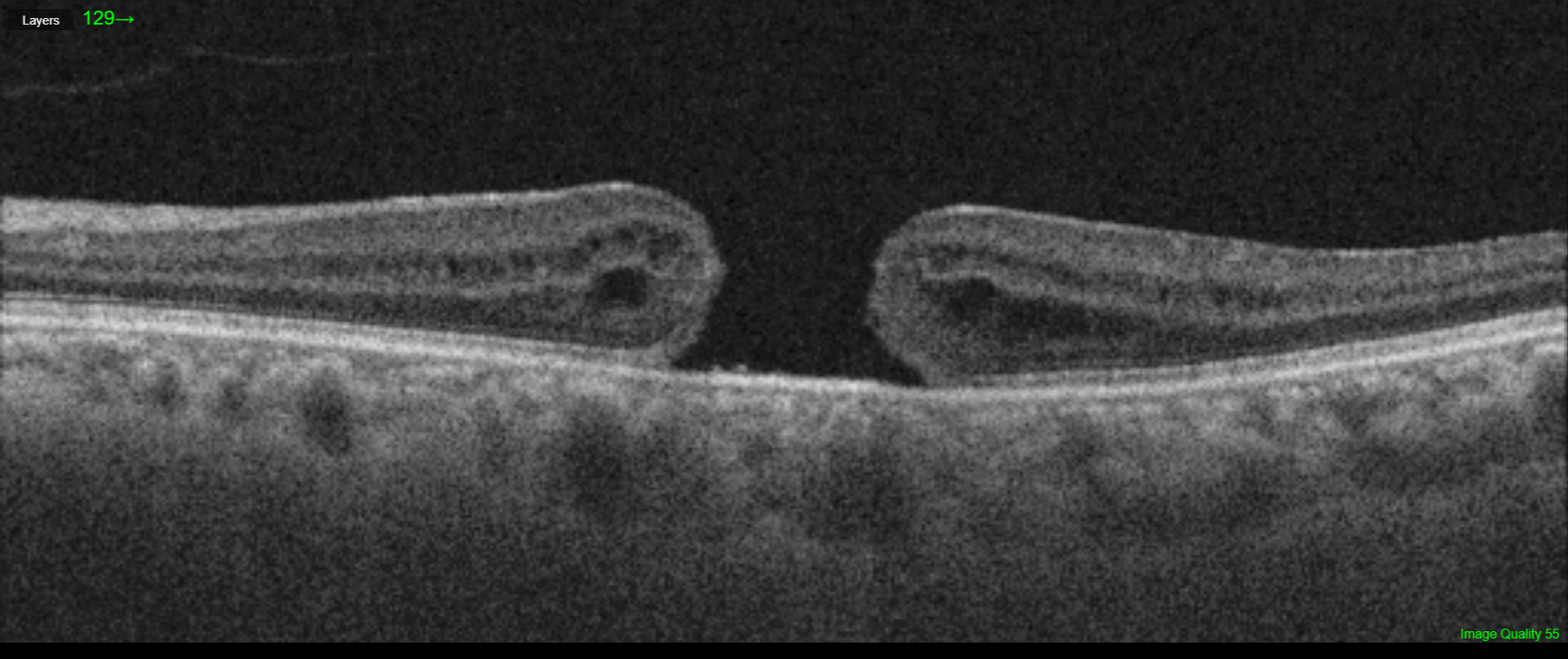
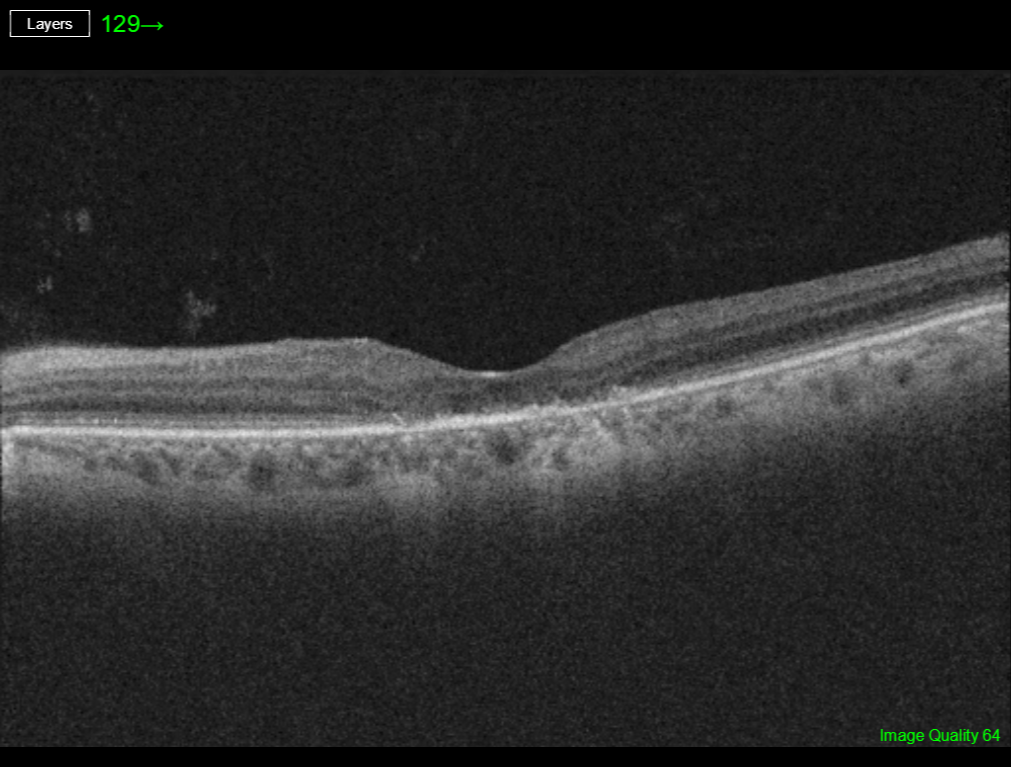
. OCT scanning through the superior lesion shows a mostly hyporeflective elevation of the neurosensory retina, with shaggy hyperreflective material along the posterior edge of the outer segments (red line/box). OCT scanning through the inferior lesion shows hyperreflective layering of the vitelliform material (yellow line/box). Similar findings were noted in their left eye (not shown). Best disease is associated with a mutation in the BEST1 gene, which encodes for the bestrophin-1 protein. Bestrophin-1, a calcium-activated chloride channel, is primarily found in the basolateral plasma membrane of the RPE. BEST1 mutations cause a variety of phenotypes, also including autosomal recessive bestrophinopathy, best vitelliform macular dystrophy, and autosomal dominant vitreoretinochoroidopathy. Our patient has progressed to the ‘scrambled egg’ appearance. The remaining vitelliform material gravitates inferiorly, often leaving an optically empty, hyporeflective space between the RPE and outer retina. Eventually the retina flattens over time with secondary outer retinal atrophy.")

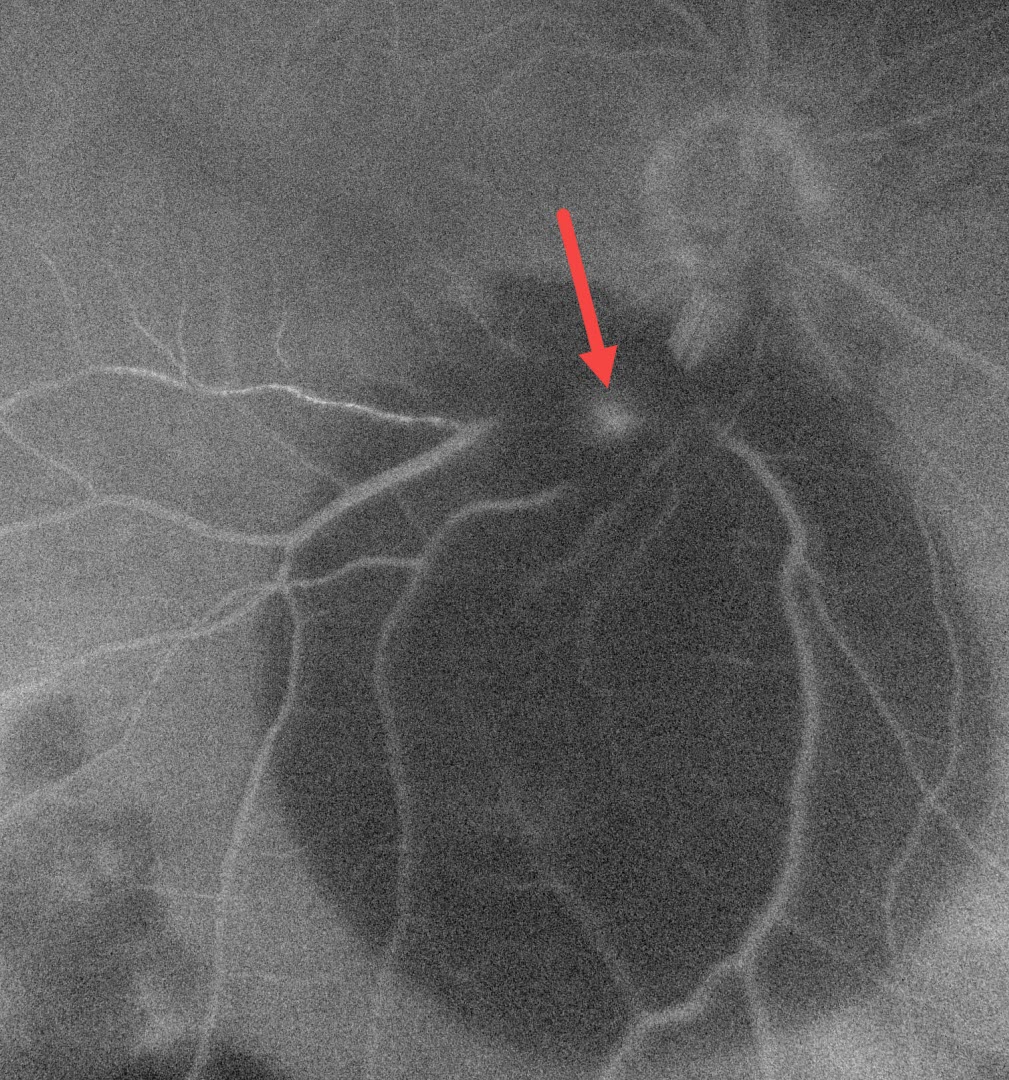
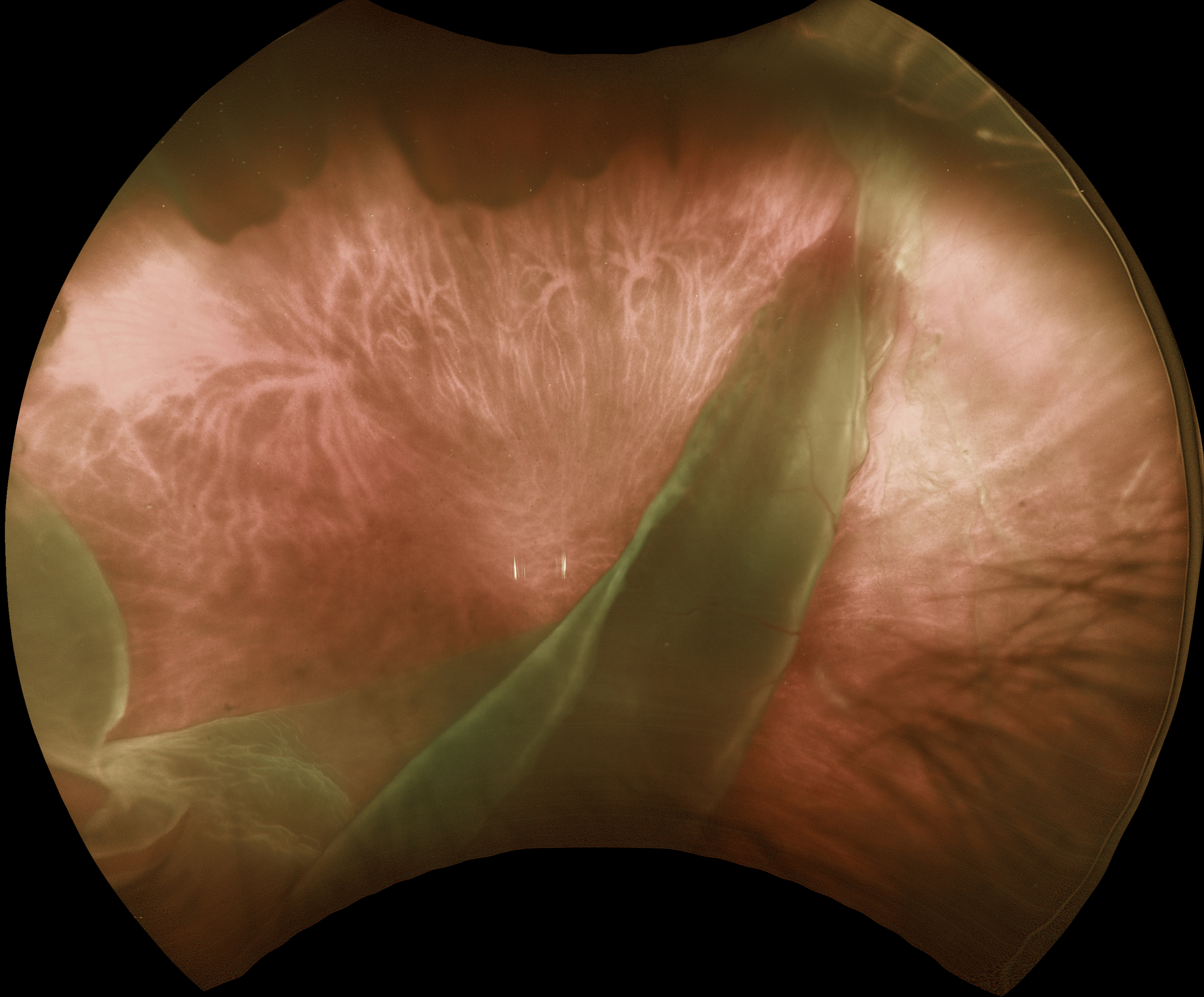
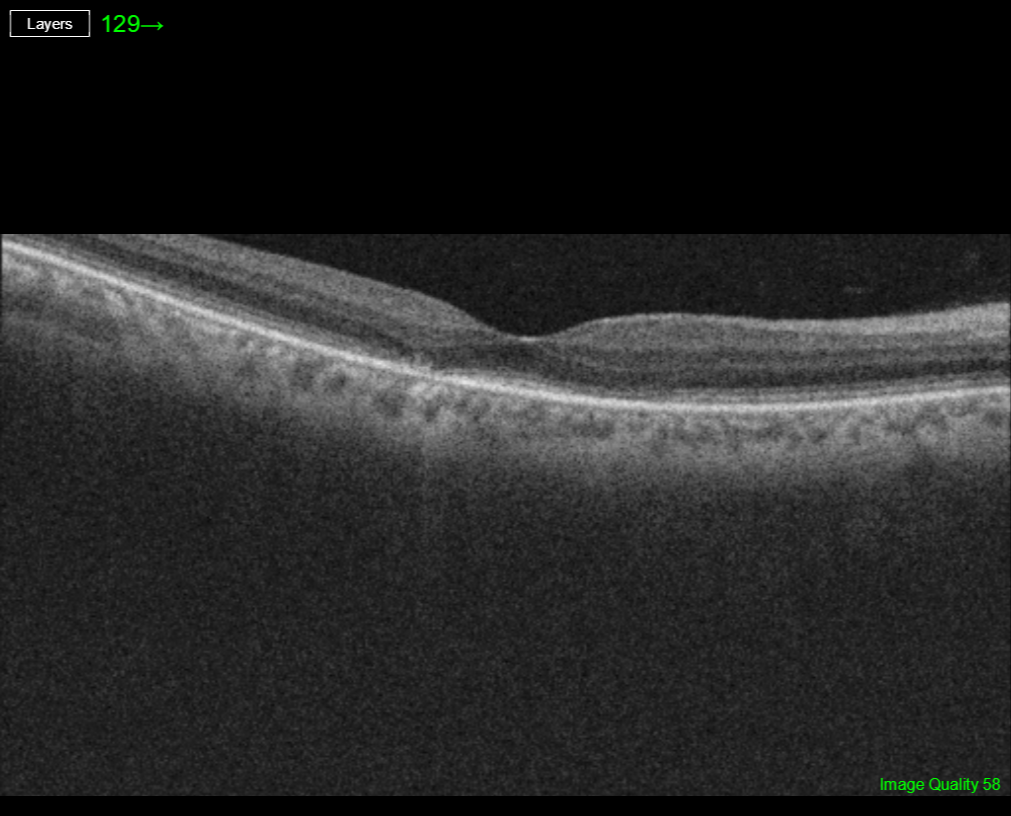
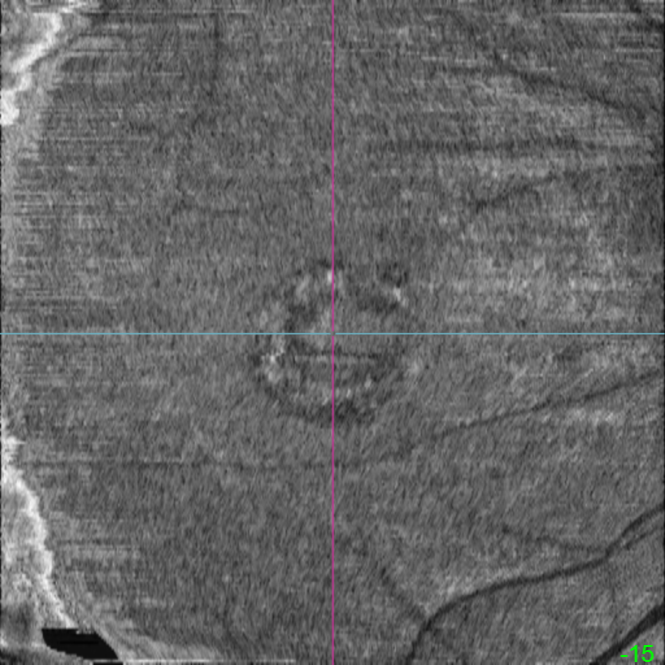
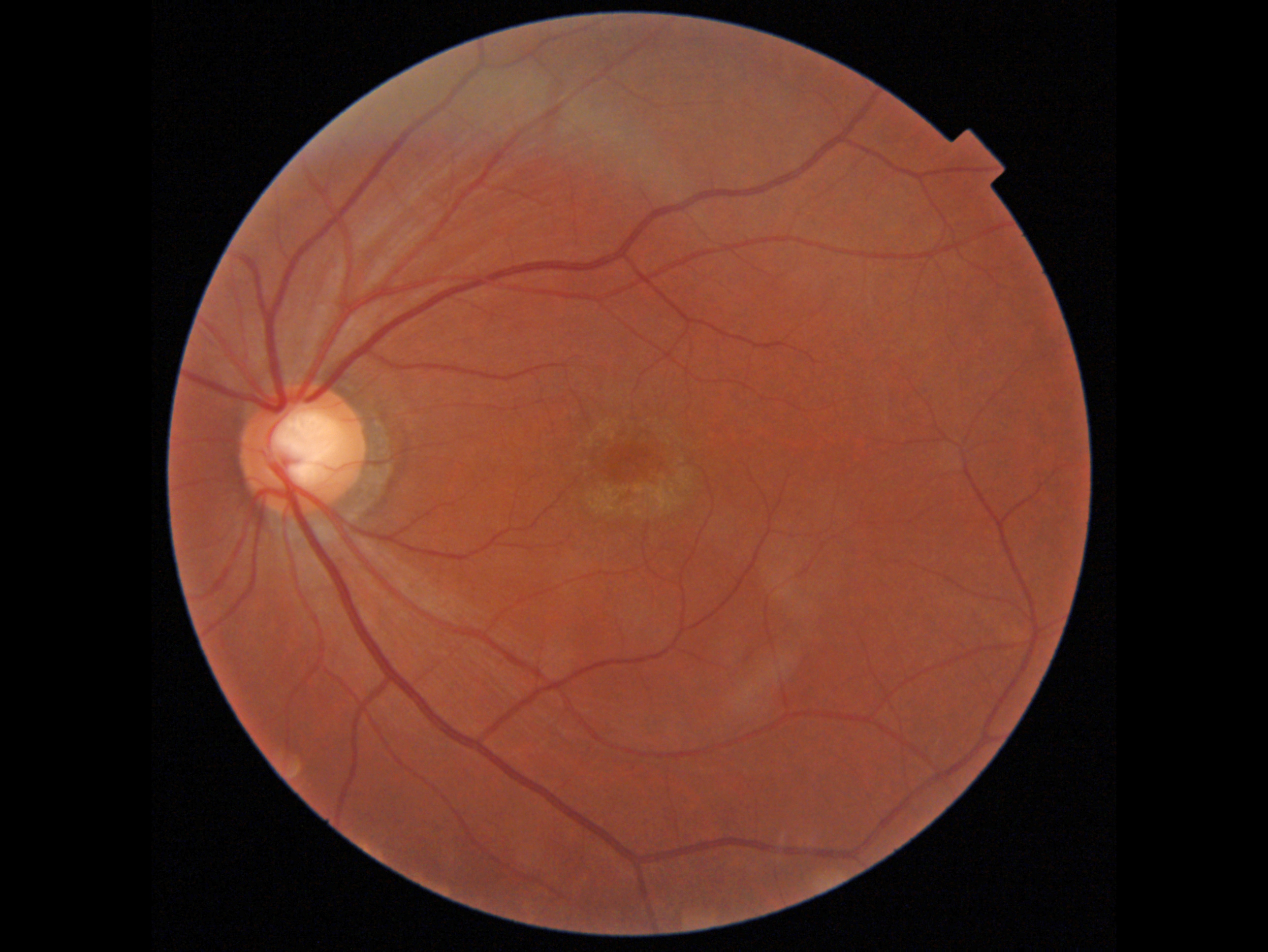
. The patient was immediately taken to surgery for corneal wound repair, lensectomy, and vitrectomy. Intraoperative photography shows a metallic intraocular foreign body (IOFB) resting just superior to the optic nerve (image 1). The impact site is just inferior to the optic nerve, with an inferotemporal branch retinal artery occlusion (BRAO) distally. The IOFB was removed with a rare earth magnet. Two weeks following surgery, vision was 20/120 with an aphakic correction. The inferior retina remains opaque, and the OCT shows inner retinal hyperreflectivity from the BRAO (image 2). A secondary intraocular lens implantation was performed 3 months postoperatively. Eleven months following the initial surgery, the BRAO is fully resolved, and secondary retinal striae extend outwards from the impact site (image 3). Vision remarkably improved to 20/30.")


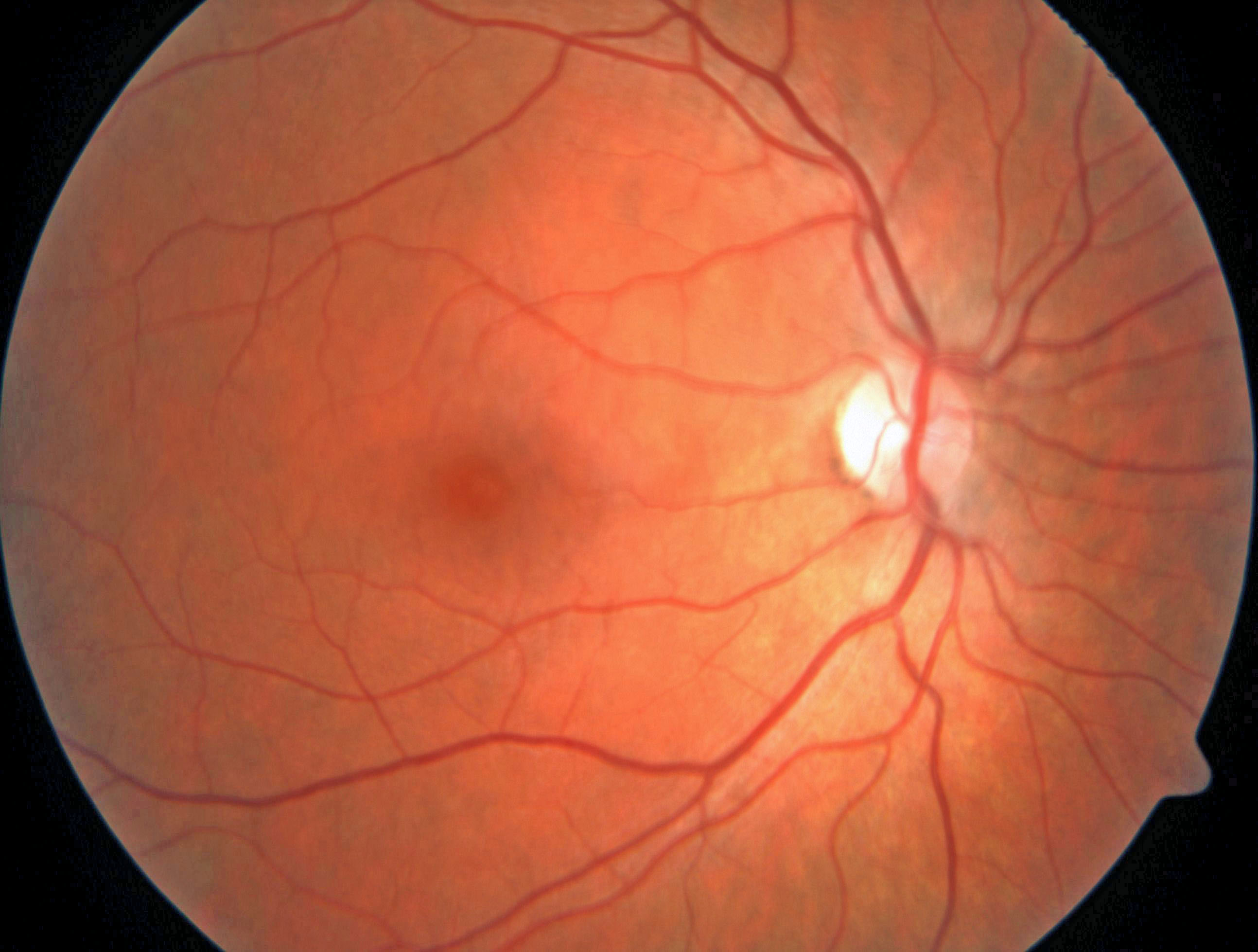
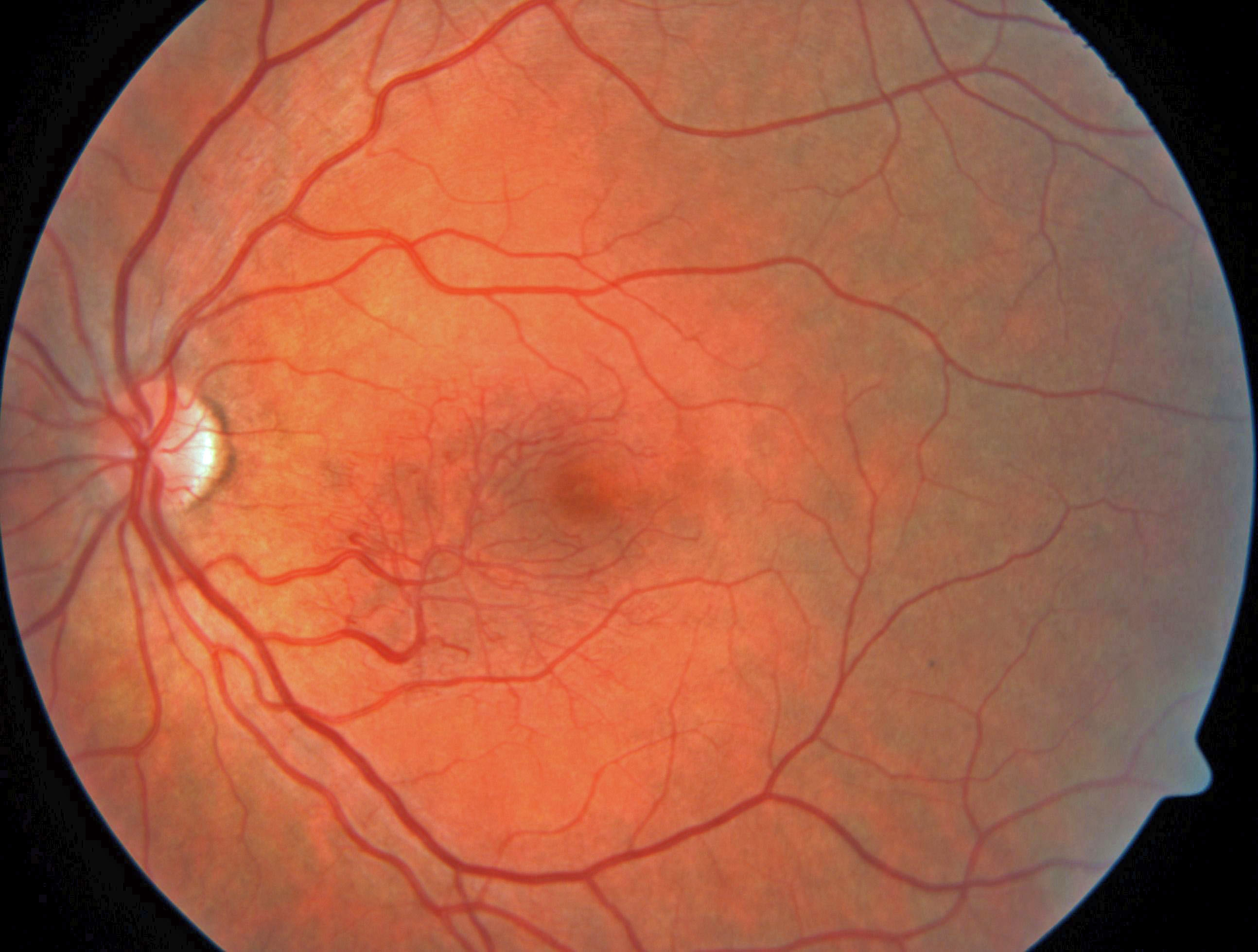
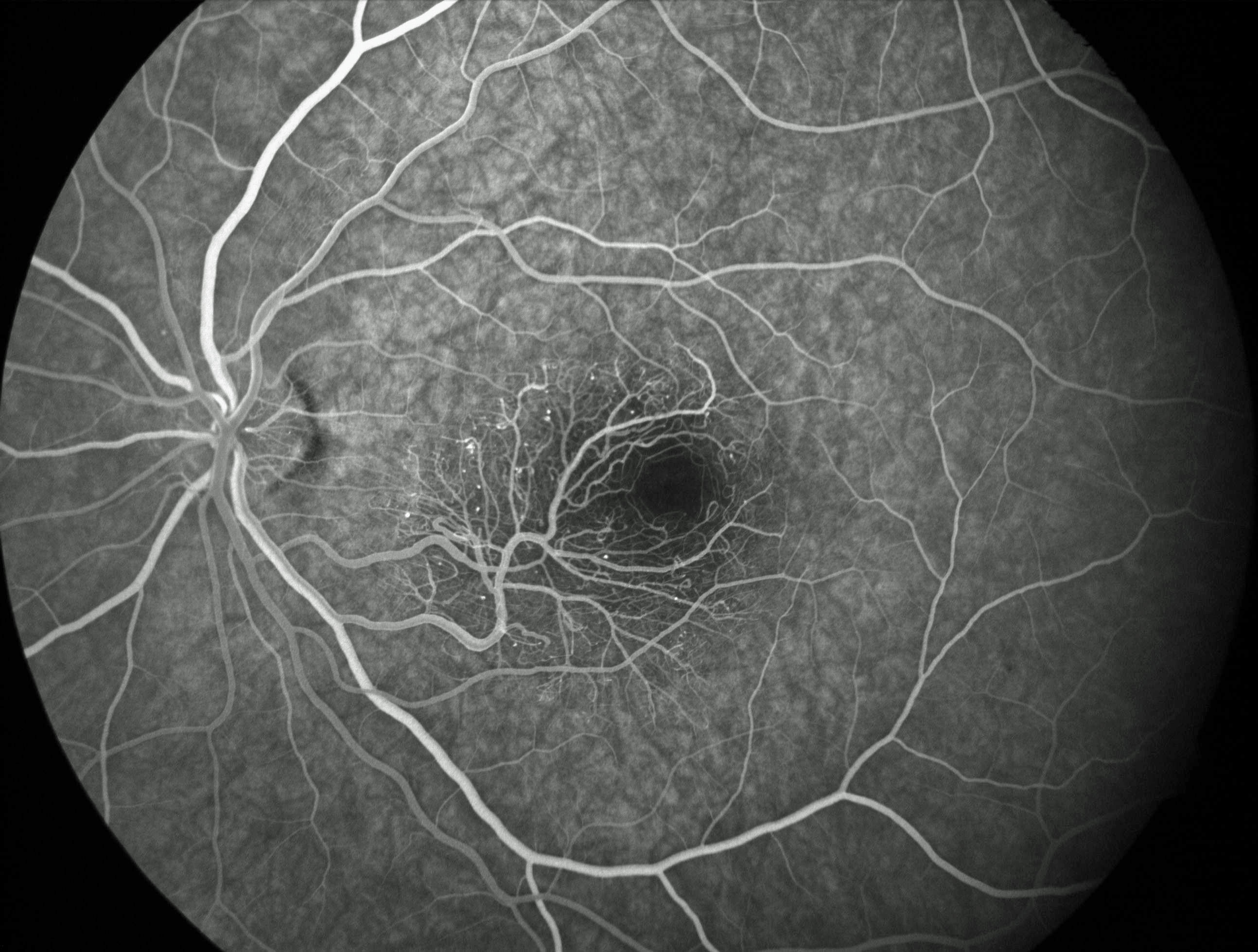
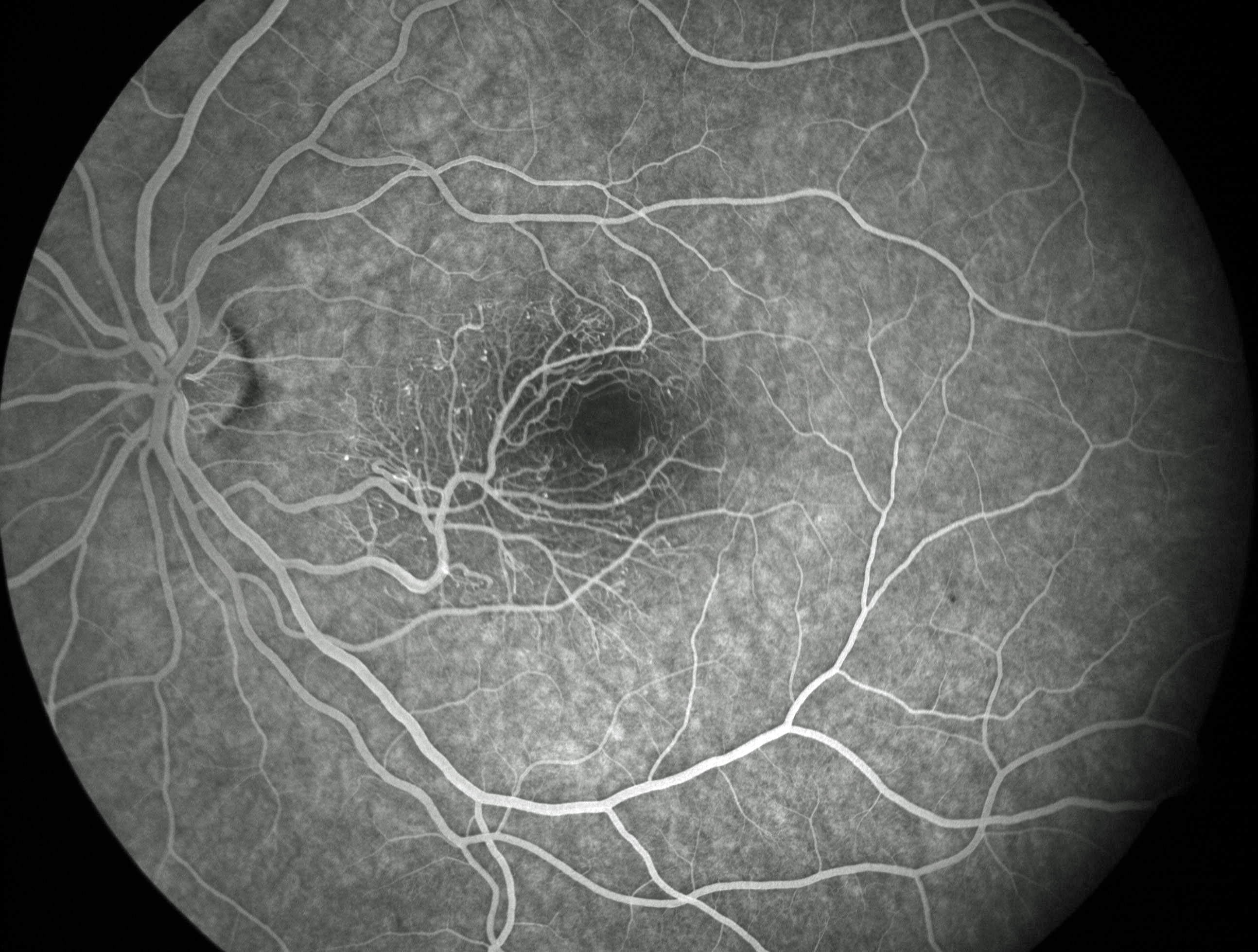
. She was referred to her oncologist. Leukemia with central nervous system involvement can rarely present with leukemic optic nerve infiltration. This can masquerade as papilledema (bilateral swollen nerves from elevated intracranial pressure) or nerve edema from inflammatory or infectious causes (Miller et al, Graefe's 2021;259:1315-1322).")


 with secondary macular neovascularization OD and lattice degeneration OU presented with new floaters in his right eye. He was scheduled for an anti-VEGF injection for the right eye on a treat-and-extend protocol the same day. Vision was stable at 20/100 OD and 20/20 OS. An acute related retinal tear was found which was immediately demarcated with thermal laser photocoagulation. Optos color RG imaging immediately following the laser procedure shows the retinal break to be well-surrounded with multiple nearly confluent rows of laser burns. The flap of the tear consists of an entire lattice lesion (green arrow) along with a chronic atrophic hole with surrounding pigment (yellow arrow). There is an area of central macular atrophy from the ICSC. Lattice lesions have a pocket of liquefied vitreous overlying thinned retina with a firm area of surrounding vitreoretinal adhesion. White, fibrosed vessels often crisscross the lesions, which lead to the name, lattice. This firm vitreoretinal adhesion, along with the often-present atrophic holes, is what can predispose these eyes to retinal breaks and detachment. Although prophylactic treatment is rarely needed, symptomatic breaks as in our patient need prompt retinopexy.")
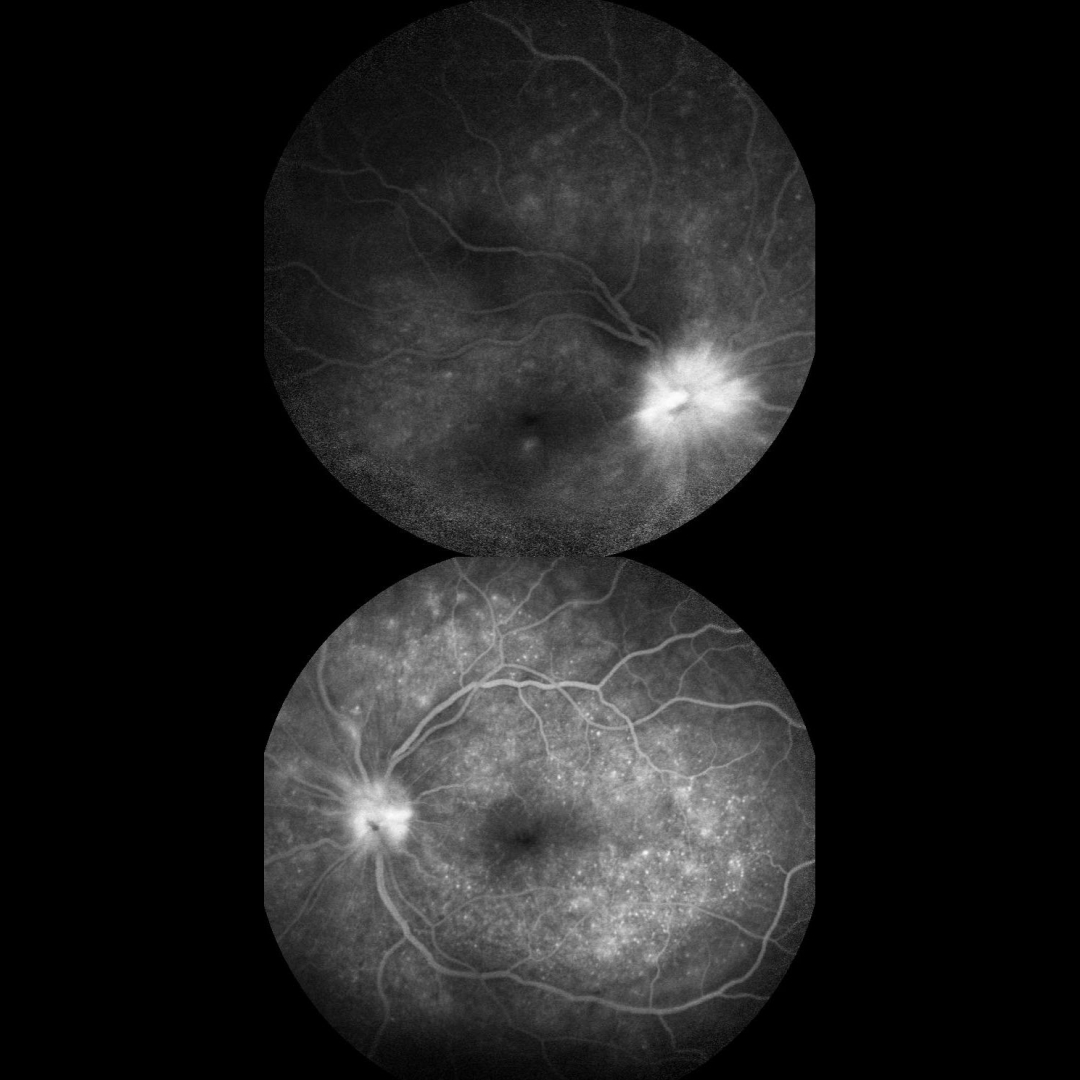
. A foveal hemorrhage is noted in the right macula. More mottled pigmented scarring extends into the right inferior periphery. OCT scanning shows variable bilateral outer retinal atrophy and hyperreflective subretinal fibrosis with mild outer nuclear cysts in the nasal left macula (images 1 and 2, bottom). This scarring stains angiographically (image 3). We were hesitant to start anti-VEGF therapy in a young boy and felt that the macular neovascularization causing the right macular blood might be inflammatory. He was therefore placed on a rapidly tapering course of oral prednisone. When last examined 6 months later, vision remained stable at 20/200 in this eye with resolution of the blood (image 4). Mantoux skin testing was negative. We have made multiple attempts to have the patient get QuantiFERON-TB Gold testing, but to date have been unsuccessful. Serpiginous choroiditis is an idiopathic, usually bilateral chorioretinal inflammatory condition usually found in middle-aged men (Khanamiri and Rao, Surv Ophthalmology 2013;58:203-232). Recurrent areas of inflammation develop along the edge of a previous scar, producing scarring that meanders from the optic nerve outwards. Vision is good unless scarring or macular neovascularization extends through the macular center. Tubercular serpiginous-like choroiditis mimics serpiginous but affects younger patients with more multifocal and peripheral recurrences and progression if untreated (Agarwal et al, AJO 2020;220:160-169). Although the exact mechanism is not yet clear, a direct or indirect infectious trigger by the Mycobacterium tuberculosis is thought to cause the choroiditis. We believe that our patient has this diagnosis and will continue to try to confirm this with further testing.")



 was of extremely poor quality, and possibly shows superior and temporal hyper-FAF just outside each macula (image 3). It was quite difficult to obtain imaging in our patient, and these studies required multiple sessions. Unfortunately, we do not have a specific diagnosis for our patient’s presumed sporadic inherited retinal disease (IRD). The location and bilaterality of the multimodal findings suggest a cone-mediated disorder. Our patient’s funduscopic appearance somewhat resembles that found in autosomal recessive CDH3 disease which includes sparse scalp hair and occasional limb abnormalities (Hull et al, JAMA Ophthalmol 2916;134:992-1000), which were absent in out patient. Genetic testing could not be performed due to cost constraints.")


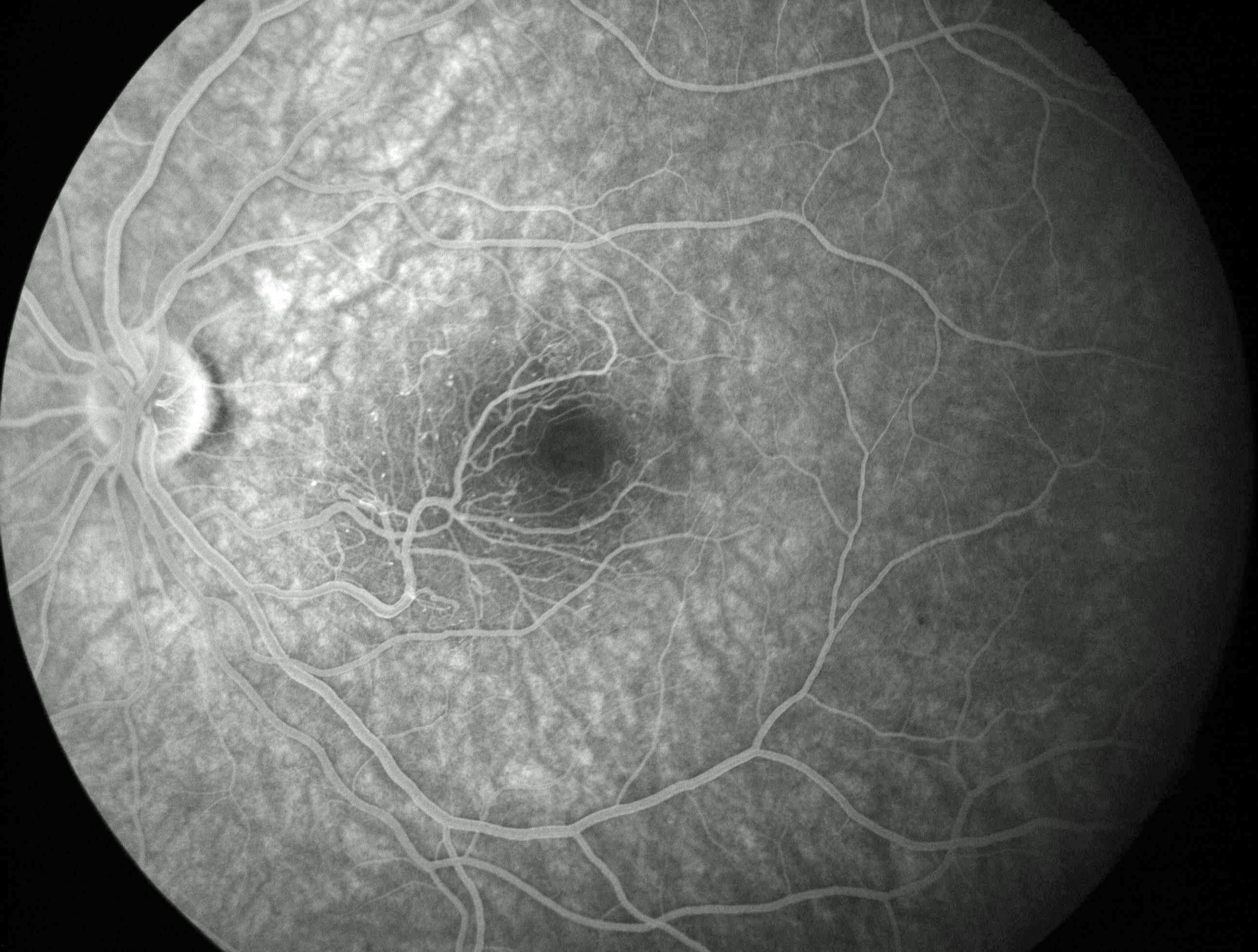
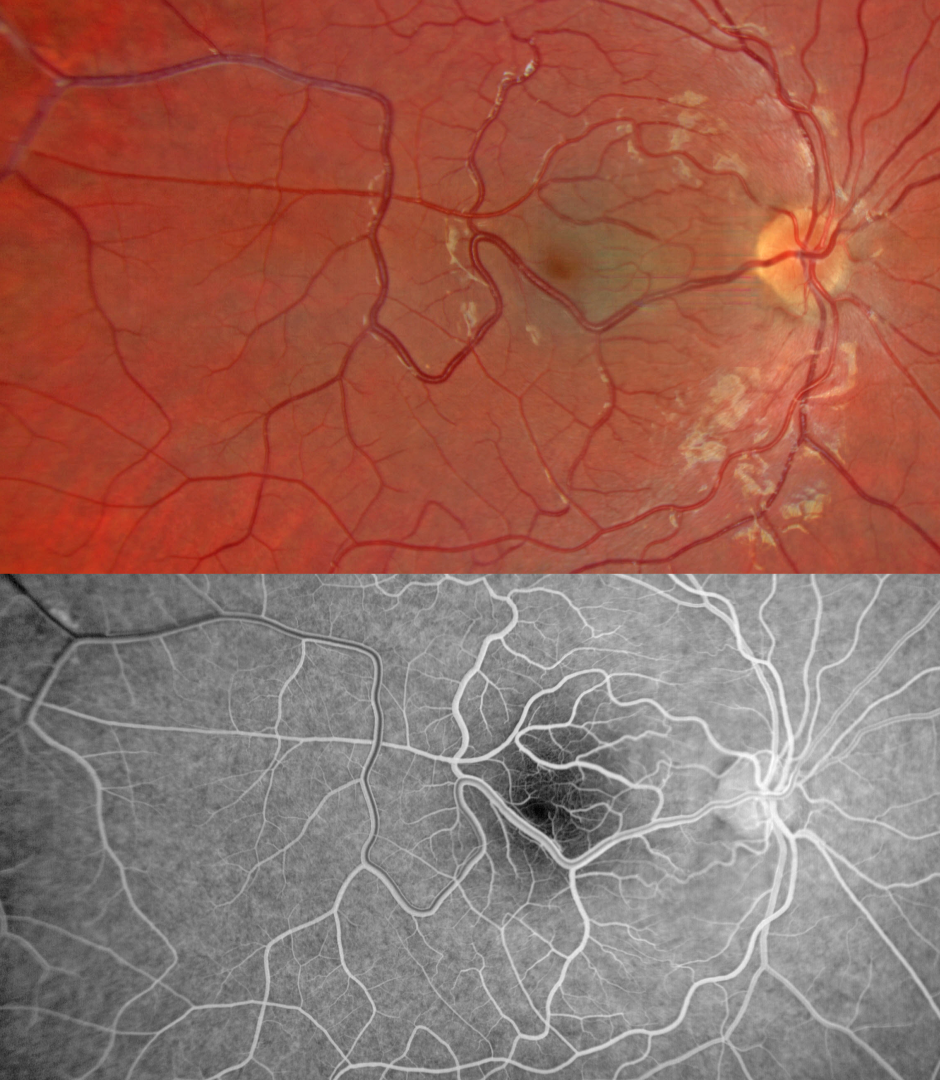
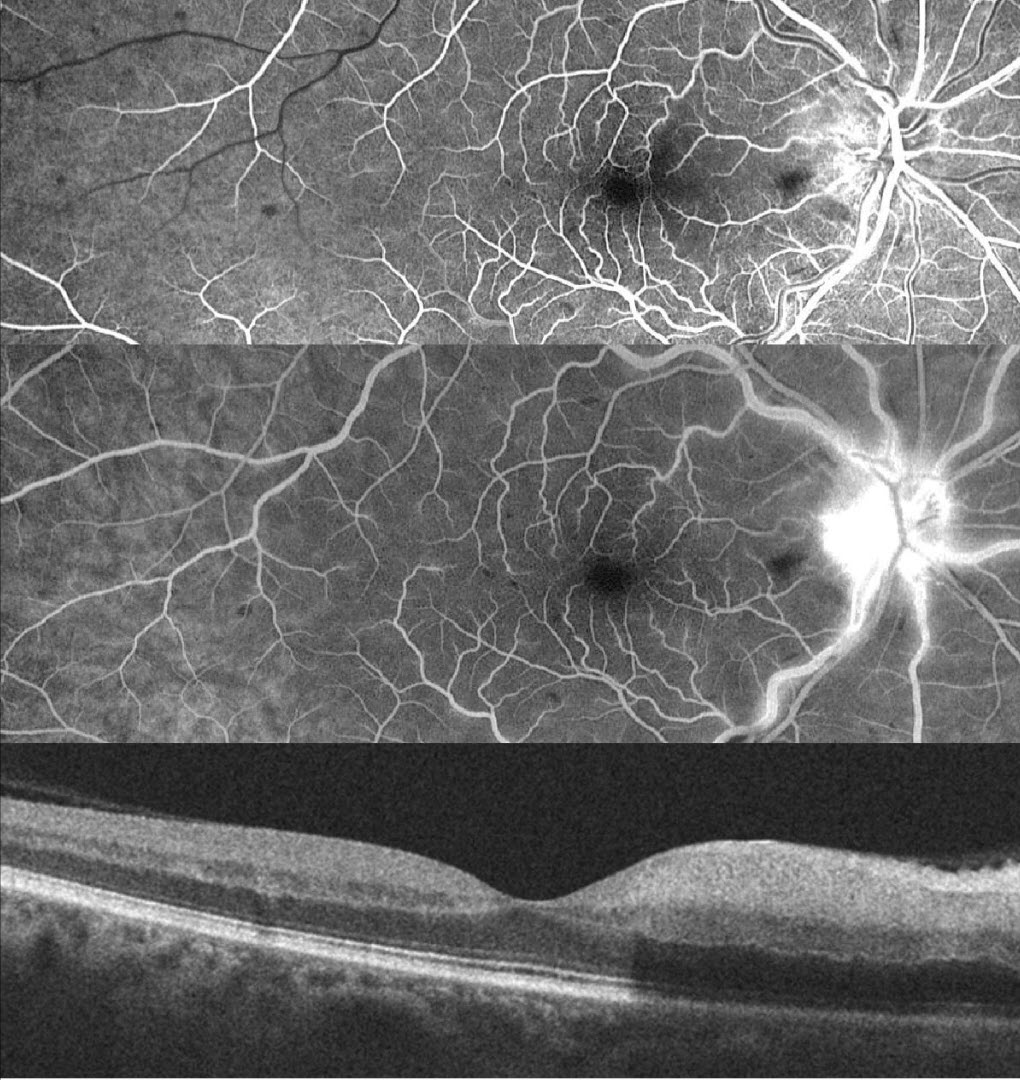
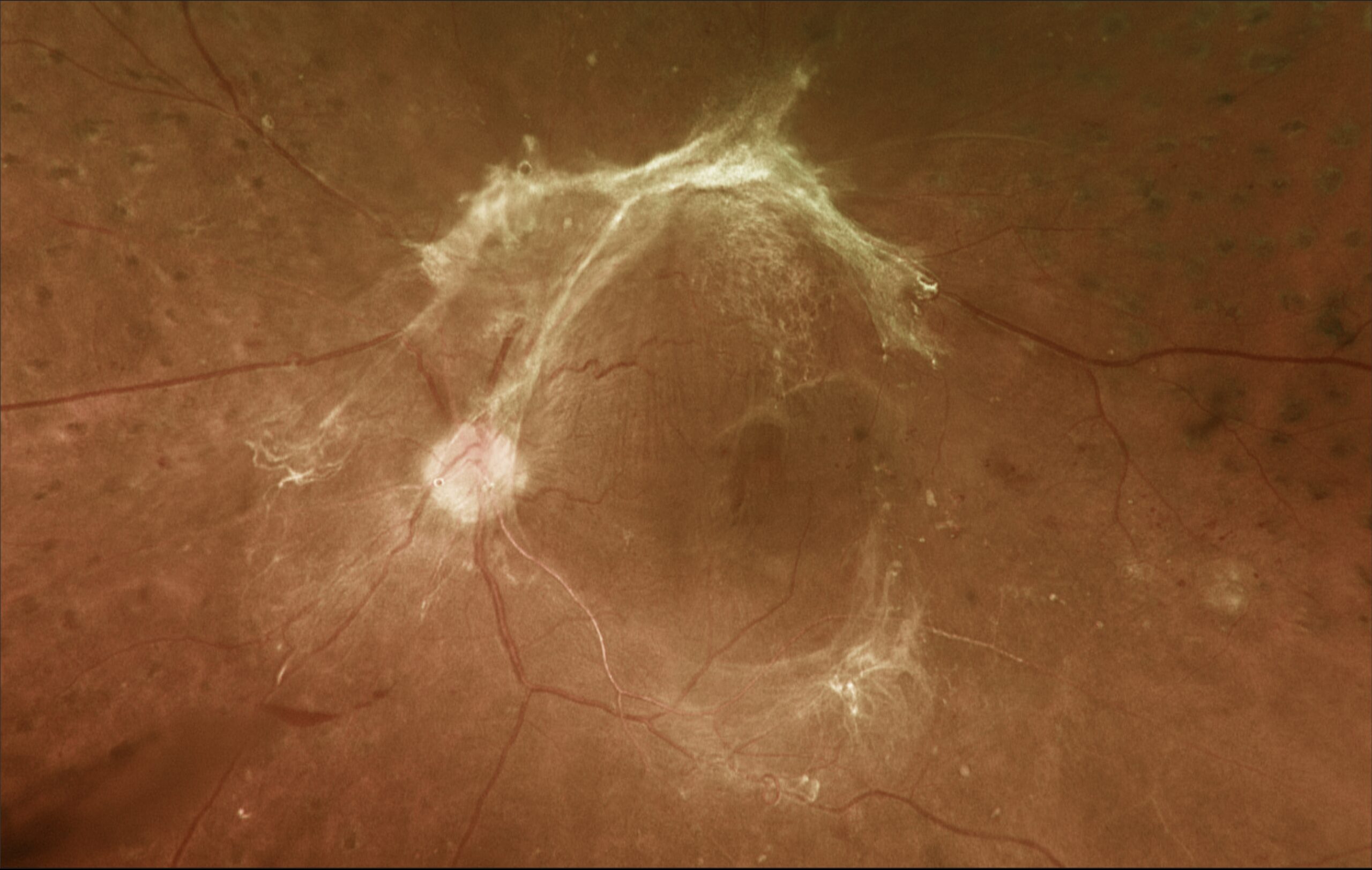
. The retinal vessels elsewhere are also somewhat dilated and tortuous. OCT scanning through the inferior macula shows these hyperreflective vessels to variably extend through full thickness retina with posterior shadowing (image 1, bottom). The early phase fluorescein angiogram showed rapid filling of the dilated artery and vein without intervening capillaries (not shown). The later phase angiogram shows no angiographic leakage (image 2). The right eye was normal (not shown). A retinal arteriovenous malformation (AVM) is a congenital connection between an artery and vein without an intervening capillary network. These lesions appear along a spectrum ranging from small isolated lesions to the large ‘bag of worms’ appearance as seen in our patient. These more extensive lesions are usually part of the Wyburn-Mason Syndrome which includes vascular lesions in the eyes and midbrain. Retinal venous malformations, aka retinal macrovessels, are now thought to represent an AVM (Pichi et al JAMA Ophthalmol 2018;136:372-379). Our patient’s MRI was fortunately normal. The AVM should likely remain stable throughout life and not require any treatment.")


. A patch of inferior lattice is also noted OD. On fundus autofluorescence, these flecks show marked hyper-FAF (image 2, bottom). On OCT, the flecks appear as hyperreflective outer retinal deposits that extend into and distort the overlying ellipsoid zone (image 3, box). Initially reported by Aish and Dajani (BJO 1980;64;652-659), benign familial fleck retina (BFFR) is an extremely rare autosomal recessive disorder that belongs to a heterogeneous group of flecked retina syndromes. The BFFR gene encodes for a group V phospholipase A2 (PLA2G5). Despite the dramatic fundus appearance, affected individuals have normal acuity, visual fields, and retinal function including electrophysiology. Other flecked retinal disorders include fundus albipunctatus, fundus flavimaculatus, familial drusen, retinitis punctata albescens, and fleck retina of Kandori. These disorders can be associated with night blindness, central visual problems, abnormal ERG, and abnormal perimetry. The ERG helps to distinguish BFFR from other flecked retina syndromes such as retinitis punctata albescens and fundus albipunctatus as scotopic ERG responses would be decreased in the later conditions but normal in BFFR.")

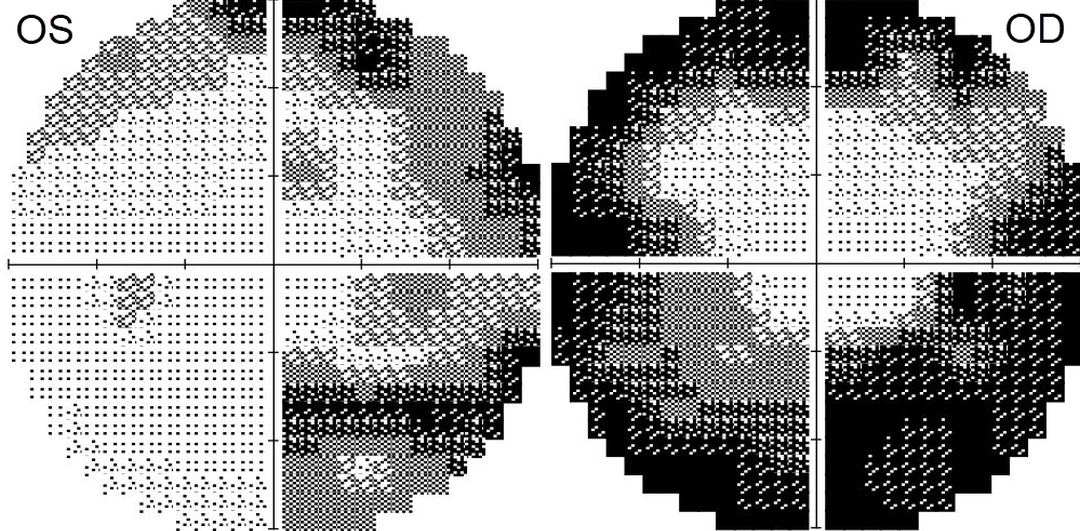
. This vessel shows angiographic laminar filling without leakage (image 2, bottom). The right and left nerves were clinically normal, and the left fundus was normal (not shown). OCT retinal nerve fiber layer analysis was normal bilaterally. Visual fields show moderate generalized constriction OD and nasal loss OS with a possible vertical cut inferiorly (image 3). Subsequent neurologic imaging was consistent with optic neuritis. Additional work up was unremarkable and neuro-ophthalmic consultation led to the diagnosis of bilateral retrobulbar optic neuritis secondary to COVID-19. Observation was recommended and symptoms started improving within a week. Two months later, all visual symptoms resolved, vision returned to 20/25 OU, and the visual fields normalized. Retinal vessels virtually always respect the horizontal meridian. Retinal venous malformations are congenital anomalous vessels that by definition cross the horizontal. Originally described by Gary Brown et al as congenital retinal macrovessels (Arch Ophthalmology 1982;100:1430-1436), these vessels are usually located in the macular region and are virtually always venous. These lesions are now called retinal venous malformations since about one-quarter of patients will have associated venous anomalies in the brain (Pichi et al JAMA Ophthalmol 2018;136:372-379).")
. Choroidal colobomas are caused by failure of the optic vesicle and choroidal fissure to close during fetal development. Choroidal coloboma can present as solitary or multiple lesions. Visual prognosis depends on the location and involvement of the optic nerve and macula. We will follow our patient yearly due to her increased risk of retinal detachment, and expect she should do well given the normal central macular appearance.")
 shows an acute central retinal artery occlusion (CRAO) with sparing of the central and inferior macula due to a large cilioretinal artery (blue arrow). The vertical OCT B-scan shows opaque hyperreflective paracentral inner retina (yellow arrows) with normal central and inferior foveal layers. Fluorescein angiography confirms preserved central and inferior macular arterial flow (image 2). Workup elsewhere included a normal brain MRI and cardiac 2D Echo. Carotid Doppler showed a plaque in the right internal carotid artery. The inner two-thirds of the neurosensory retina is supplied by the central retinal artery, with the choroid supplying the RPE and photoreceptor layer. Acute CRAO therefore presents with white edematous inner retina that spares the fovea. Cilioretinal arteries, which arise from the posterior choroidal circulation, are present in up to 50% of individuals, and bilateral in about 25% (Schneider et al, Acta Ophthalmologica 2021;99:e310-e318). Our patient was quite fortunate to have a large cilioretinal vessel that relatively preserved central vision. Patients with acute retinal ischemia (defined as transient monocular vision loss, acute BRAO or acute CRAO) need to be emergently referred to a stroke center. This is especially urgent with an acute CRAO since about 75% of patients have already developed a recent stroke. If the patient presents immediately following the occlusion, measures to acutely lower the intraocular pressure in attempt to move the causative embolus downstream can be performed, including ocular massage, paracentesis and breathing into a bag. Unfortunately most patients present outside this window (Shah et al, Ophthalmology Retina 2023;7:527-531) and even then, these measures are usually ineffective.")
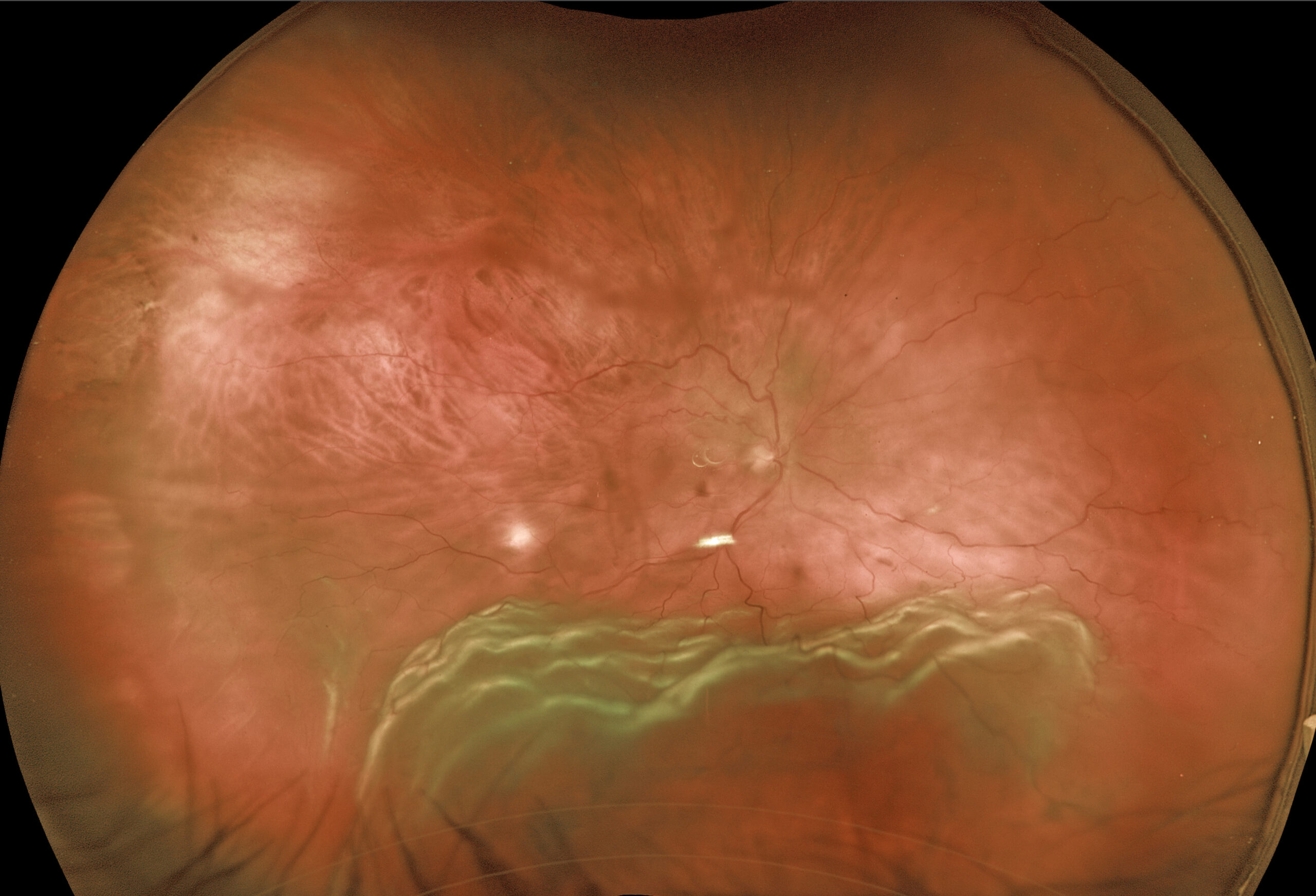
. In our office vision was 20/100 OD and 20/60 OS. Intraocular pressure (IOP) was 30mmHG. Anterior segments showed shallow anterior chambers with retrolental vitreous cells. Multicolor imaging shows bilateral irregular chorioretinal folds, multifocal serous detachments, and disc hyperemia (images 1 and 2, top). OCT scanning shows a bacillary layer detachment OD, subretinal fluid OS, and a bilateral undulating thickened choroid (images 1 and 2, bottom). Fluorescein angiography shows bilateral optic nerve and areas of pinpoint subretinal leakage (image 3). She was diagnosed with Harada’s disease and started on Intravenous methylprednisolone for 3 days followed by 60mg prednisone PO daily. She was also referred to rheumatology to start immunosuppressants. The acetazolamide was tapered and discontinued for the misdiagnosed IIH. One week later, vision improved to 20/40 OU, IOP was 10mmHG OU with marked bilateral improvement in the chorioretinal folds, macular fluid and choroidal thickening (images 4 and 5). A slow steroid taper began pending starting immunosuppressants. This case has many classic findings for Harada’s disease, including bilateral panuveitis, optic nerve swelling, thickened choroid, chorioretinal folds, and multifocal serous exudative retinal detachments. Patients with just ocular findings have Harada’s disease, whereas those with additional systemic findings (including vitiligo, poliosis, headache, vertigo, and hearing loss) have Vogt-Koyanagi-Harada (VKH) disease. This case also reminds us that it is easy to misdiagnose these complex uveitis cases, especially when all the ocular findings are not taken in total to try to give the patient a single, unifying disease.")

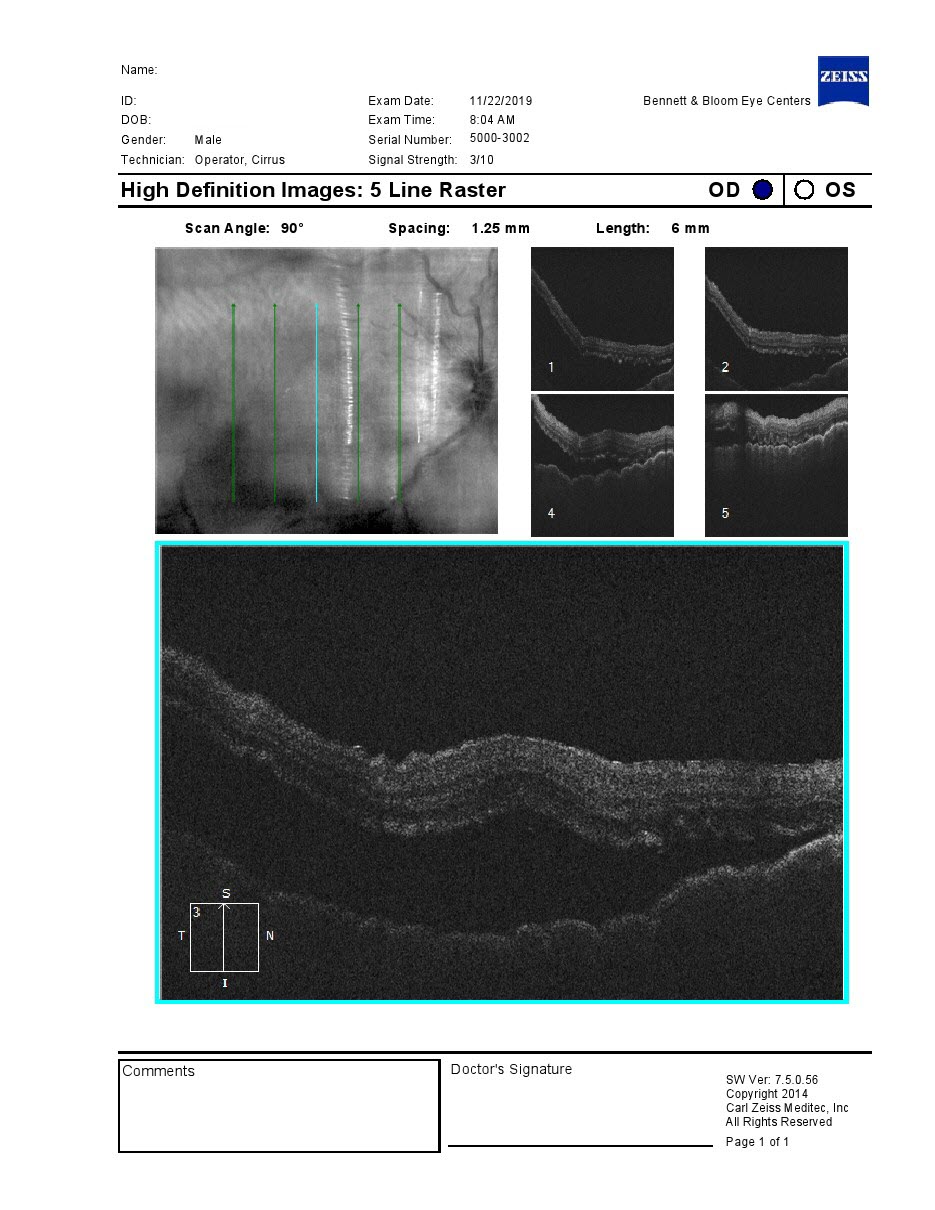
. Vision was 20/20. The patient was started on 50mg of prednisone and slowly tapered off by rheumatology. She returned on 7/19/23 with pain behind her right eye. Vision was 20/20. Color imaging shows subtle chorioretinal folds in the superior midperiphery (image, top). OCT B-scan through this region confirmed the chorioretinal folds (image, bottom) B-scan ultrasonography revealed bilateral T signs. Posterior scleritis can present either as a diffuse thickening of the entire posterior sclera or as a nodular type with localized scleral thickening (see Agrawal et al, Retina 2016;36:392-401). Nodular inflammation appears as a posterior pole subretinal yellowish mass lesion, often with overlying serous fluid and chorioretinal folds. B-scan ultrasonography may show fluid in the Tenon space (“T” sign). Unlike anterior scleritis, the eyes are usually quiet and pain-free. Initial treatment is usually with oral non-steroidal anti-inflammatories or corticosteroids, although patients may also require immunosuppressive therapy. For a large case series of posterior scleritis, see McCluskey et al, Ophthalmology 1999;106:2380-2386. Oral prednisone was restarted and slowly tapered. Further labs and chest X-ray were performed to rule out other possible causes of scleritis and she was started on Humira.")
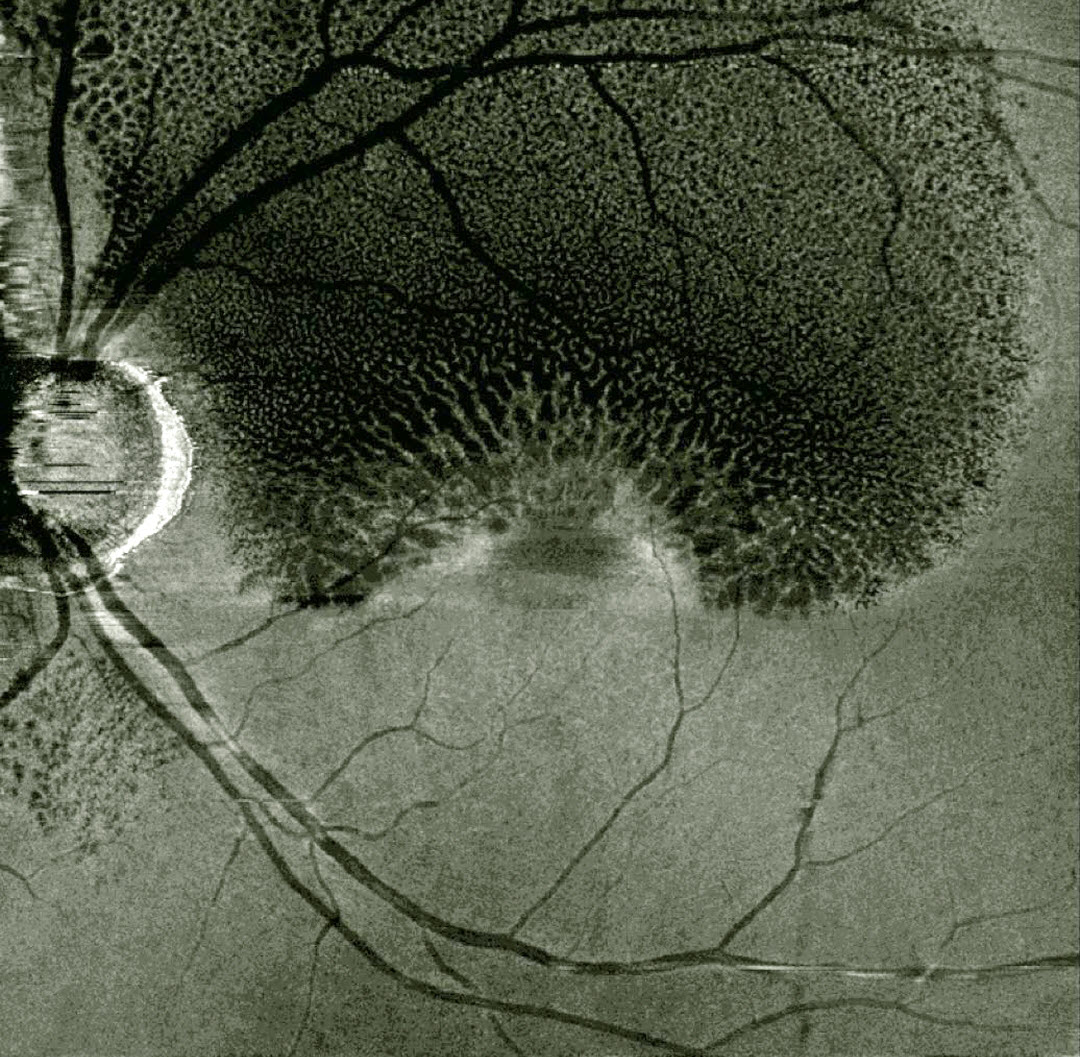
 hemorrhage obscuring his right macula. A Neodymium:YAG laser was used to create a small inferior opening in the ILM (arrow). Fundus photography shows that the blood immediately started to drain into the inferior vitreous. Valsalva retinopathy is characterized by usually unilateral retinal and preretinal hemorrhages caused by raised intrathoracic or intraabdominal pressure. Various causes include coughing, heavy lifting, and vomiting. These hemorrhages virtually always resolve without sequelae, although the sub-ILM blood in severe cases can be drained into the inferior vitreous by creating a small ILM opening using either a thermal or Nd:YAG laser as was done for this patient.")

, which are hypoautofluorescent (image 2) Similar findings were noted in her left eye (not shown). Electrophysiology and genetic testing were normal. Group-type congenital pigmented nevi of the RPE (bear tracks) is a relatively rare congenital condition characterized by well-demarcated, hyperpigmented, flat, variably sized RPE lesions, resembling bear footprints. Histopathologically, these lesions are similar to congenital hypertrophy of the RPE (CHRPE), with increased numbers of pigment granules in normal-sized RPE cells. These lesions are benign, cause no visual symptoms and are not associated with familial polyposis. The major fluorophore with fundus autofluorescence (FAF) is lipofuscin, which is intraliposomal RPE material generated as byproducts of outer segment metabolism. The outer retina overlying these bear track lesions shows varying degrees of atrophy. This leads to less lipofuscin production with hypo-FAF.")
. Optos imaging shows apparent choroidal melanocytosis temporally in her left eye (image, bottom). But in actuality, this is the only normally pigmented choroid in each eye, with diffuse choroidal hypopigmentation elsewhere. When questioned, she mentioned synophrys (fusion of the eyebrows), that she removed with LASER, poliosis that she dyed, and a family history of poliosis and heterochromia. She is also congenitally deaf. Waardenburg syndrome is a usually autosomal dominant group of genetic disorders characterized by achromia of the hair and/or skin, congenital deafness, partial or total iris heterochromia, synophrys, broad and high nasal root, telecanthus, and choroidal hypopigmentation. Vision is usually normal as was the case in our patient. See Shields at al for a review of the iris and choroidal abnormalities found in Waardenburg syndrome (JAMA Ophthalmol 2013;131:1167-1173).")
. Fluorescein angiography showed staining of these lesions (images 2 and 3, middle) with cystoid leakage in his right macula (image 2, middle). OCT scanning showed a mild epiretinal membrane with cystoid edema OD (image 2, bottom). The initial differential diagnosis included birdshot chorioretinopathy and sarcoidosis.
The initial differential diagnosis included birdshot chorioretinopathy and sarcoidosis. HLA-A29 was negative, but on further questioning he told us that the tattoos on his arms always became swollen and painful prior to the recurrent uveitis (image 1, right upper arm). A biopsy of one of the inflamed tattoos revealed inflammation granulomatosa, classified as a foreign body or sarcoid type reaction. However, sarcoidosis workup, including angiotensin converting enzyme, chest X-ray and chest computed tomography, were all normal. The uveitis continues to be treated as needed with oral and topical steroids.
Tattoo-associated uveitis presents as a bilateral granulomatous anterior or panuveitis (see Ostheimer et al, AJO 2014;158;637-643). Although the uveitis can often develop years following the tattoo placement, ocular inflammation usually occurs concurrent with raised and indurated tattoos. Skin biopsy of these inflamed lesions shows noncaseating granulomatous inflammation surrounding the tattoo pigment. This inflammation is felt to represent an immune response against the dermal pigment, and sarcoidosis is a known risk factor. The uveitis can be controlled with systemic steroids and/or immunosuppressants.")


 shows a large vertical oval of retinal elevation extending from the superior macula into the inferior midperiphery (yellow arrows). This fluid connects to an inferotemporal optic nerve pit (blue arrow). OCT scanning (bottom) shows subretinal fluid (red arrow), cystic fluid mostly in the outer nuclear layer (orange arrow), and fluid below the internal limiting membrane vs within a split nerve fiber layer (pink arrow). He was referred to a retinal specialist for further evaluation and possible treatment. An optic nerve pit is a rare (about 0.1% prevalence) congenital anomaly thought to be caused by incomplete closure of the optic fissure during gestation. Pits are most commonly located within or along the inferior-temporal disc margin and usually appear as a gray depression. While most optic pits are asymptomatic (as in this case), they can cause vision loss due to fluid being forced into the inner retina, outer retina, and finally the subretinal space (optic pit maculopathy). The source of the fluid continues to be a source of ongoing debate, coming from either the vitreous or subarachnoid space. A host of treatments for optic pit maculopathy have been suggested over the years. However, a recent meta-analysis suggested that a plain old vanilla vitrectomy without gas tamponade is as successful as any other procedure (Zheng et al Ophthalmology Retina 2020;4:289-299).")
. The beds of the RPE tears are depigmented (red arrows). Increased subretinal pigmentation is noted on either edge of the giant tear (yellow arrows). Subretinal fluid variably elevates the macula with inner retinal folds radiating from the optic nerve temporally. This subretinal fluid extends into the superior and temporal midperipheries (image 2, yellow arrows).
B-scan OCT shows marked subretinal fluid (image 1, bottom). Bare Bruch’s membrane is noted temporally (orange arrow), and the RPE tear is lifted nasally and floating within the serous detachment (pink arrow).
Fluorescein angiography (image 3) shows marked hyperfluorescent window defects from the absent RPE (red arrows) with blockage on either side of the giant tear from the redundant retracted RPE (yellow arrows). He was placed on a 5-day tapering course of oral steroids but was subsequently lost to follow-up.
An asymptomatic retinal pigment epithelial detachment (PED) is noted in his right macula (image 4, yellow arrows). The choroid does not appear thickened on OCT B-scan.
A tear of the RPE is most commonly seen in RPE detachments (PEDs) associated with neovascular AMD but can also occur in numerous other etiologies including central serous chorioretinopathy and polypoidal choroidal vasculopathy. The tear leaves a depigmented region where the RPE was and is now absent, along with a pigmented relatively straight subretinal lesion from the scrolled RPE edge.
Our patient’s presentation is unique in that RPE tears are usually much smaller and tend to rip in just one direction. The edges of our patient’s RPE retracted both nasally and temporally. RPE tears are usually singular, and ours had an additional, much smaller secondary tear more inferiorly. Although our patient’s findings seem to be in the pachychoroid spectrum, the lack of a thickened choroid on OCT scanning makes the etiology less certain. See Ersoz et al for a great review on RPE tear classification, pathogenesis, predictors and management (Surv Ophthalmology 2017;62:493-505).")
. A few small areas of more distal red subretinal blood are seen (green arrow). An inferior macular branch retinal artery occlusion (red arrow) likely accounted for her symptoms. The blood column is stagnant within the inferior portion of the acute occlusion (blue arrow). OCT thickness map shows inferior and inferonasal thickening that just spares the foveal center (inset). A B-scan through the BRAO (image 1, bottom) shows hyperreflective inner retina (pink arrow) with subretinal fluid (orange arrow). OCT through the macular center was relatively normal (not shown). Fluorescein angiography (image 2) shows blockage from the subretinal blood, along with a leaking retinal arterial macroaneurysm (RAM, red arrow).
In this case, we felt that the BRAO was secondary to mechanical arterial compression from the surrounding blood. An intravitreal Avastin injection was therefore given in hopes of improving the exudation and decompressing the artery.
Vision was 20/40 one month later. Thin red subretinal blood surrounds a larger round mound of yellowing, devitalized blood (image 3). OCT thickness map shows inferior macular atrophy from the prior BRAO (inset). A B-scan through the foveal center is relatively normal (image 2, bottom).
This case is from Retina Rocks (www.retinarocks.org, @retina.rocks), one of the world’s largest online, open-source retina image teaching resources and the image bank for the Retina World Congress. Anyone interested in helping contribute to and grow the platform should contact Steve Bloom at smbloo01@gmail.com.")

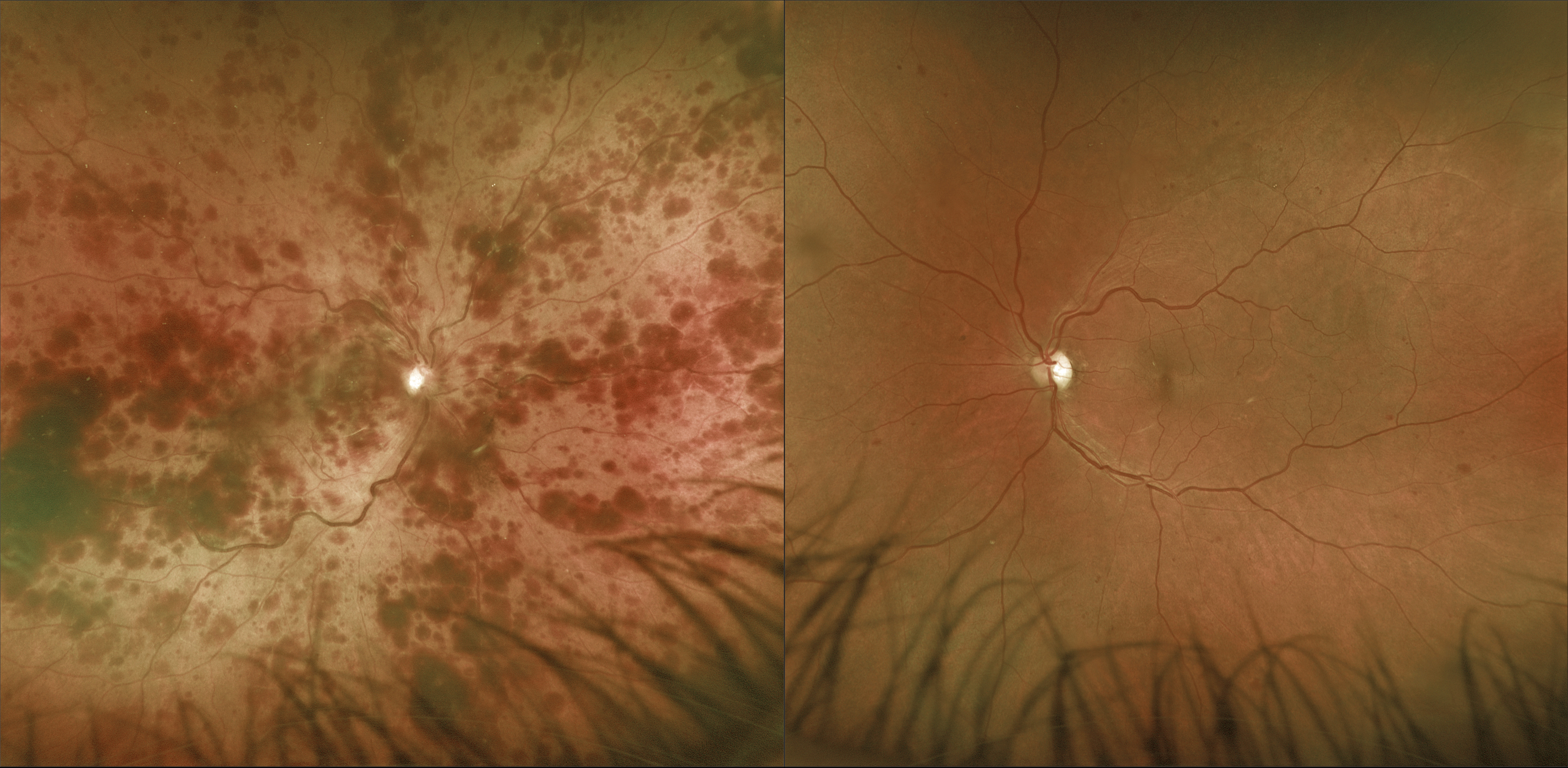
 with mild scattered retinal hemorrhages in all quadrants (image 1). There is an acute nasal macular branch retinal artery occlusion (BRAO), likely secondary to the CRVO. A small round patch of congenital hypertrophy of the RPE (CHRPE) is present superotemporally, and two patches of myelinated nerve fiber layer (NFL) are seen nasally. Fluorescein angiography shows a well-perfused central retinal vein occlusion (CRVO) with late optic nerve leakage (image 2, top and middle). OCT scanning shows nasal inner retinal hyperreflectivity (image 2, bottom).")
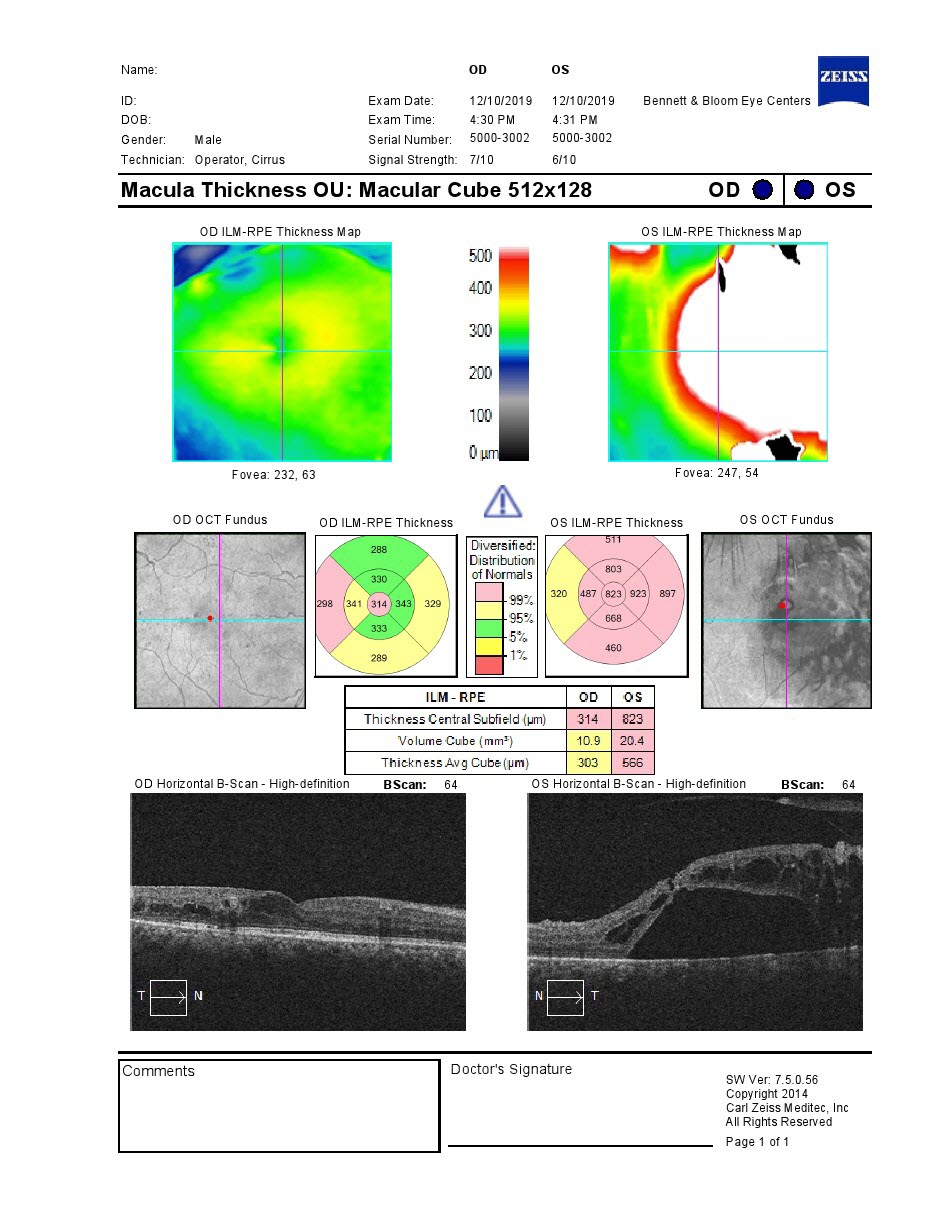
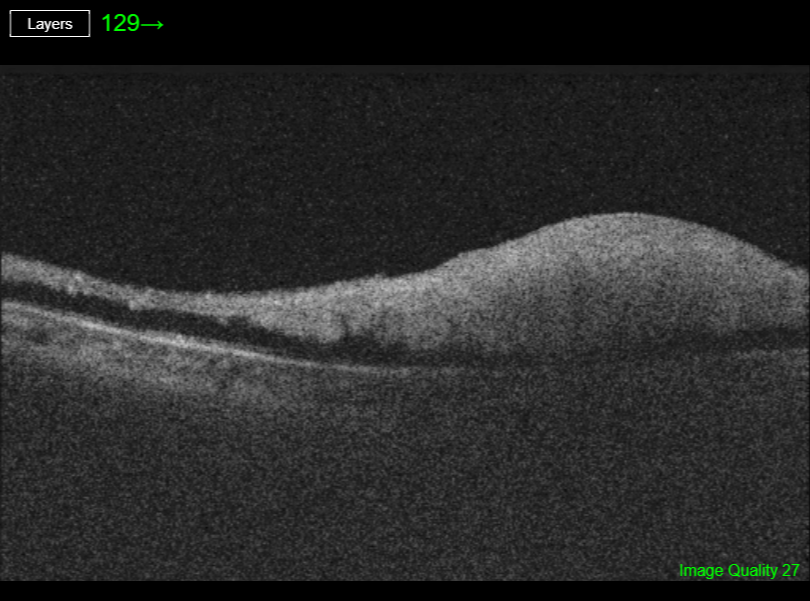
. Widefield OCT shows an elevated hyporeflective choroidal mass with overlying cystic retinal edema (image 1, bottom, yellow arrow). Subfoveal fluid (orange arrow) with cystic fluid in the outer retina (pink arrow) is noted in the macula. An en face OCT of the outer retina more dramatically shows the cystic changes (image 2). The choroidal lesion with overlying retinal edema dramatically improved following photodynamic therapy (image 3). Vision improved to 20/20. Widefield imaging is revolutionizing the way we diagnose and treat retinal disease. This case is a perfect example where macular imaging alone could point to an incorrect diagnosis. In this case the macular findings in isolation suggest either optic pit maculopathy (Imamura et al, Retina 2010;30:1104-1112) or paraproteinemic maculopathy (Mansour et al, Ophthalmology 2014;121:1925-1932). This technology led to a correct diagnosis, allowing for appropriate treatment with excellent anatomic and visual results.")

. Despite the vitreous blood, we were able to adequately visualize the causative break (image 1, arrow) and surround it with cryotherapy. A week later, the vitreous hemorrhage increased and vitrectomy was performed. At the time of surgery, the vitreoretinal traction on the causative tear and blood vessel was relieved. The retina was attached without other breaks. Vision improved to 20/20 five days postoperatively.")
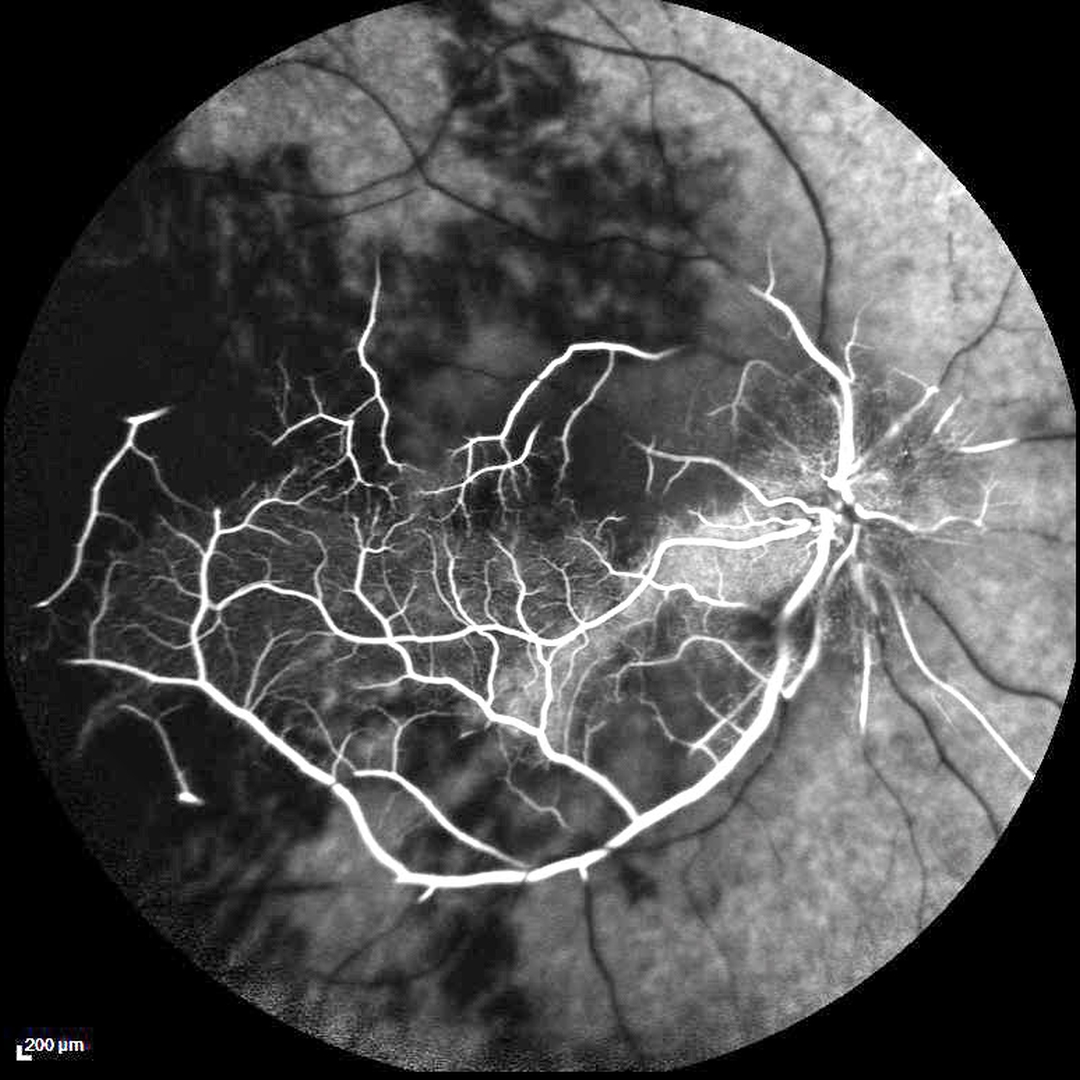
. Vision was 20/20 OU. Color imaging shows large temporal nonperfused retinal vessels with old inferior yellow vitreous hemorrhage (image 1 and image 2, top). The retinal vessels are diffusely dilated and tortuous. OCT B-scan shows a remarkably normal central macula with some distal inner retinal thinning (image 2, bottom, arrow). Fluorescein angiography confirms widespread peripheral nonperfusion (image 3). Anti-VEGF therapy followed by panretinal photocoagulation was given. The Central Vein Occlusion Study (CVOS) defined ischemic CRVO as having at least 10 disc areas of angiographic retinal nonperfusion as determined by standard photographic views with the Canon (60 degrees) or Topcon (45 degrees) wide-angle fundus cameras (Ophthalmology 1995;102:1434-1444). Although clearly ischemic, this patient might have been classified by the CVOS as a perfused occlusion depending on how much of the temporal ischemia would have been imaged. As with diabetic retinopathy (see Brucker, Retina 2021;41:461-463), ultrawidefield imaging and anti-VEGF injections have thrown a literal wrench into how we think about, classify, and treat retinal disorders.")

. There is a small dot of central blood (arrow). Swept-source OCT (image 1, bottom) shows a markedly thickened choroid (yellow line) with variable regions of hyper- and hyporeflectivity. A hyperreflective type 2 macular neovascularization (MNV) is seen (red arrow) along with exudative subretinal fluid (green arrow). OCT angiography shows flow signals within the MNV (image 2, arrow). B scan ultrasonography shows the lesion to be markedly hyperreflective (image 3, arrow). An anti-VEGF injection was given, but she was unfortunately subsequently lost to follow-up. Choroidal osteomas are benign, calcified amelanotic choroidal tumors. They are more common in women, almost always unilateral and usually located in the peripapillary or macular regions. Being a choroidal lesion, they are best seen on the Optos red channel Fluorescein angiography (FA) usually shows early patchy hyperfluorescence with late diffuse staining. Ultrasonography is often helpful in differentiating an osteoma (markedly hyperreflective) from other amelanotic choroidal tumors. Macular neovascularization develops in a significant number of eyes and can be successfully treated with anti-VEGF therapy (see Seong et al, Graefe’s 2022;250:1713-1721).")

. Triton imaging of the optic nerve coloboma shows optic nerve pits temporally and nasally (image 2, top, arrows). Swept source OCT dramatically reveals the pits (image 2, bottom). We are following him yearly. Both optic nerve and choroidal colobomas can be unilateral or bilateral and are caused by incomplete closure of the embryonic fissure. Patients with choroidal colobomas are at a lifetime increased risk for rhegmatogenous retinal detachment due to breaks that occur in the overlying thinned retina. Optic nerve pits are also associated with serous macular detachment and macular neovascularization. For a great review of cavitary optic nerve abnormalities, see Jain and Johnson, AJO 2014;158:423-435.")
. Swept-source OCT shows bilateral ellipsoid zone and outer segment defects (images 1 and 2, bottom, red arrows). We diagnosed him with the ACHOO reflex (Autosomal Dominant Compelling Helioophthalmic Outburst). And yes, that is a real thing! Patients with this entity sneeze when exposed to bright lights, typically sunlight. The outer retinal damage in solar retinopathy is thought to be caused by photochemical outer retinal and RPE damage instead of a thermal burn. Vision is usually fairly good despite the outer retinal and RPE findings. We advised him to stop his sun gazing ritual, although we’re not sure this will be possible for him.")
. The detachment was successfully repaired with vitrectomy surgery. Her asymptomatic left eye showed extensive temporal lattice lesions with atrophic holes (image 2), and prophylactic laser was recommended.")
, measuring 407 microns. There was also a moderately severe nuclear sclerotic cataract. Combined cataract surgery with 23-gauge pars plana vitrectomy, temporal half-moon inverted ILM flap and fluid-air-SF6 exchange was performed followed by prone positioning. On the 5th postoperative day, the flap extended over the closed hole, but one week later the ILM flap retracted and was scrolled onto itself, suspended anterior to the macula. Three weeks following vitrectomy, the hole completely flattened with partial restoration of the outer retinal layers. The ILM flap continued to contract and scroll onto itself. Vision was 20/40. Introduced by Kelly and Wendel (Arch Ophthalmol 1991;109:654-659), macular hole surgery is one of the modern success stories in ophthalmology. ILM flaps appear to improve the surgical success for large macular holes. In this case, the ILM flap inadvertently scrolled onto itself and away from the macular hole by postoperative day 12. Some authors have suggested that the ILM flap provides a scaffold for cells to grow over and help heal the hole. However, most macular holes are actually foveal dehiscences without tissue loss, where the foveal retina splits and elevates like a drawbridge (Tornambe, Retina 2003;23:421-424). For successful surgery, there is thus no need or significant evidence for glial or neurosensory retina regrowth, just for the “drawbridge” to close. As this case exemplifies, most likely the ILM flap serves the same purpose as the gas bubble, sealing the macular hole from the overlying liquid vitreous. This allows the RPE to actively pump (and the choroid to passively absorb) the subretinal fluid allowing the foveal tissue to flatten into its normal position. Once the hole closes, if the vitreous and epimacular traction are relieved, there is likely no need for the ILM flap.")

 Complete pars plana vitrectomy, 2) Creation of a temporal retinal detachment, 3) Peripheral 200 degree retinotomy, 4) Macular neovascularization (MNV) removal, 5) Feeder vessel endodiathermy, 6) Designing the peripheral choroidal patch with endodiathermy, 7) Cutting and isolation of a full thickness autologous RPE and choroid transplant (under perfluorocarbon liquid, PFCL), 8) Translocation of the patch under the fovea (under PFCL), 9) Transfer of PFCL from under to over the retina with retinal reattachment, 10) Peripheral laser and 11) PVCL exchange for 1000cs silicone oil. Eight years later, Clarus 500 widefield photography shows the intact submacular choroidal autograft and the white area of bare sclera in the temporal quadrant which was the harvesting site of the autograft (image 1). Canon Xephilio S1 widefield OCT shows fairly normal retina overlying the graft. Xephilio A1 angioOCT shows the intact choroidal graft vessels arranged in a different direction compared to the native surrounding choroidal vasculature (image 2). When last examined near vision was 20/30. She recently developed a MNV in the contralateral eye which is being treated with anti-VEGF injections.")
. Optic pits are most commonly located within or along the inferior-temporal disc margin and usually appear as a gray depression. They are thought to be caused by incomplete closure of the optic fissure during gestation. While most optic pits are asymptomatic (as in this case), they can cause vision loss due to fluid being forced into the inner retina, outer retina, and finally the subretinal space (optic pit maculopathy). The source of the fluid continues to be a source of ongoing debate, coming from either the vitreous or subarachnoid space. This case can be found on www.retinarocks.org, in the Image Library, Optic nerve (ON) pit folder, ON pit HXS-.")
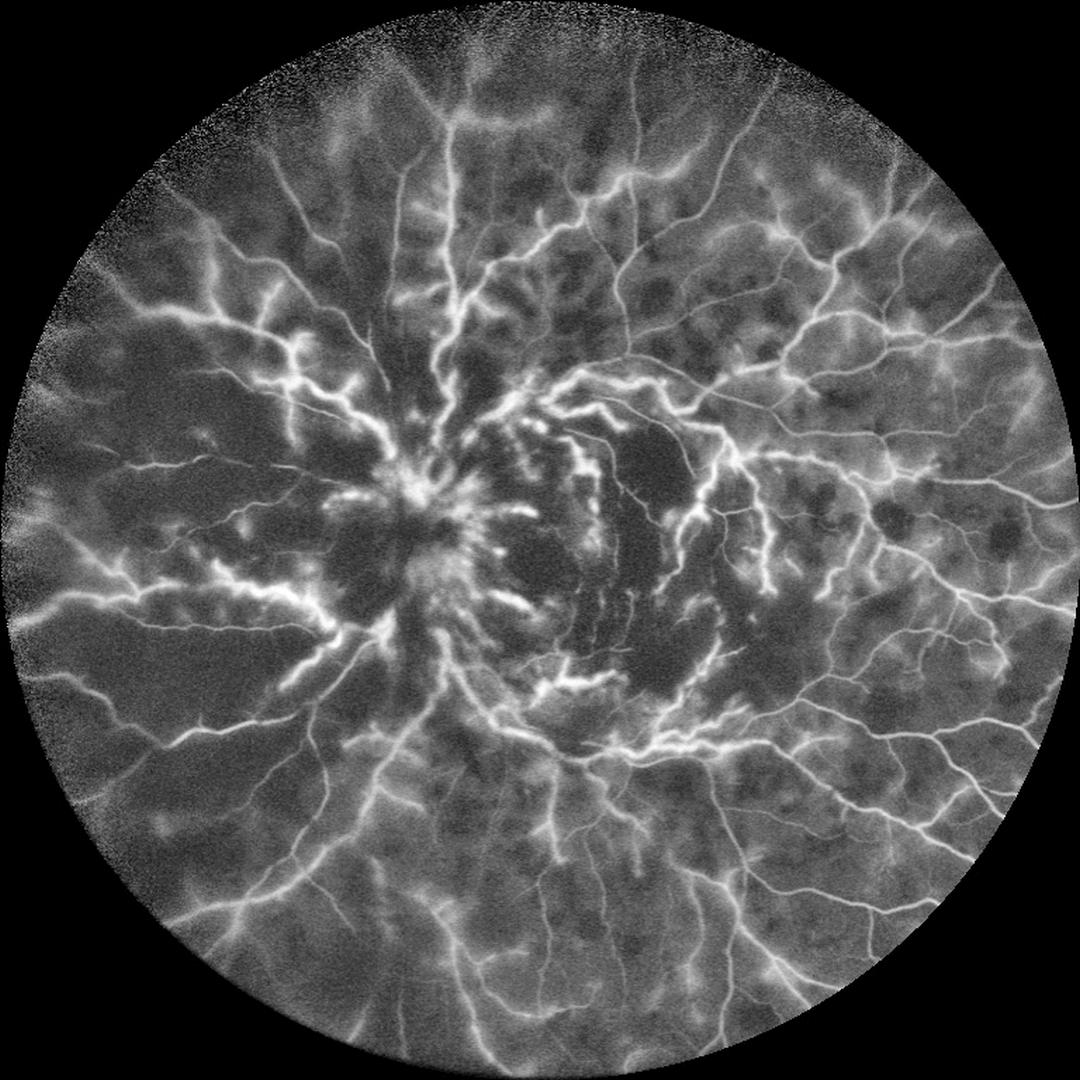
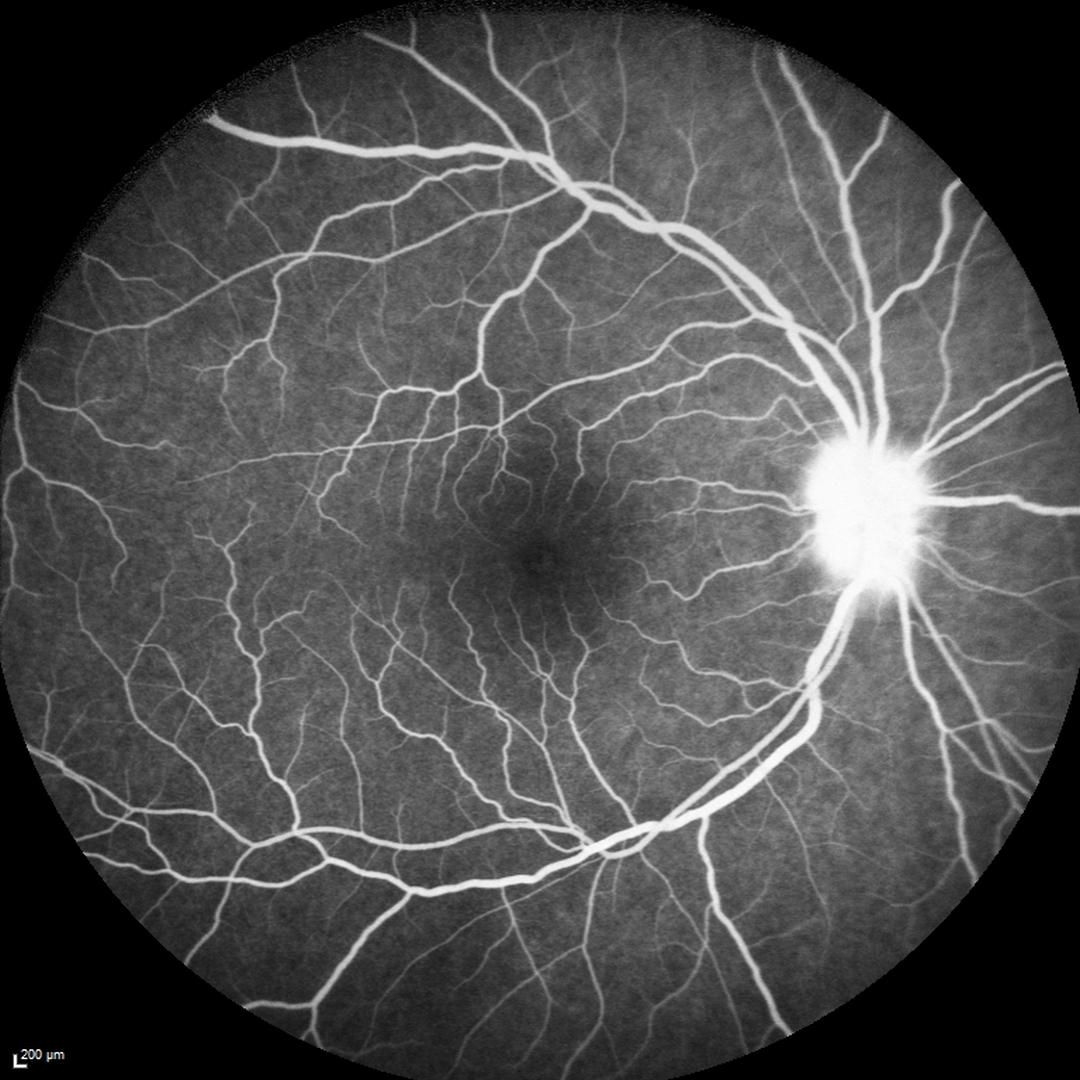
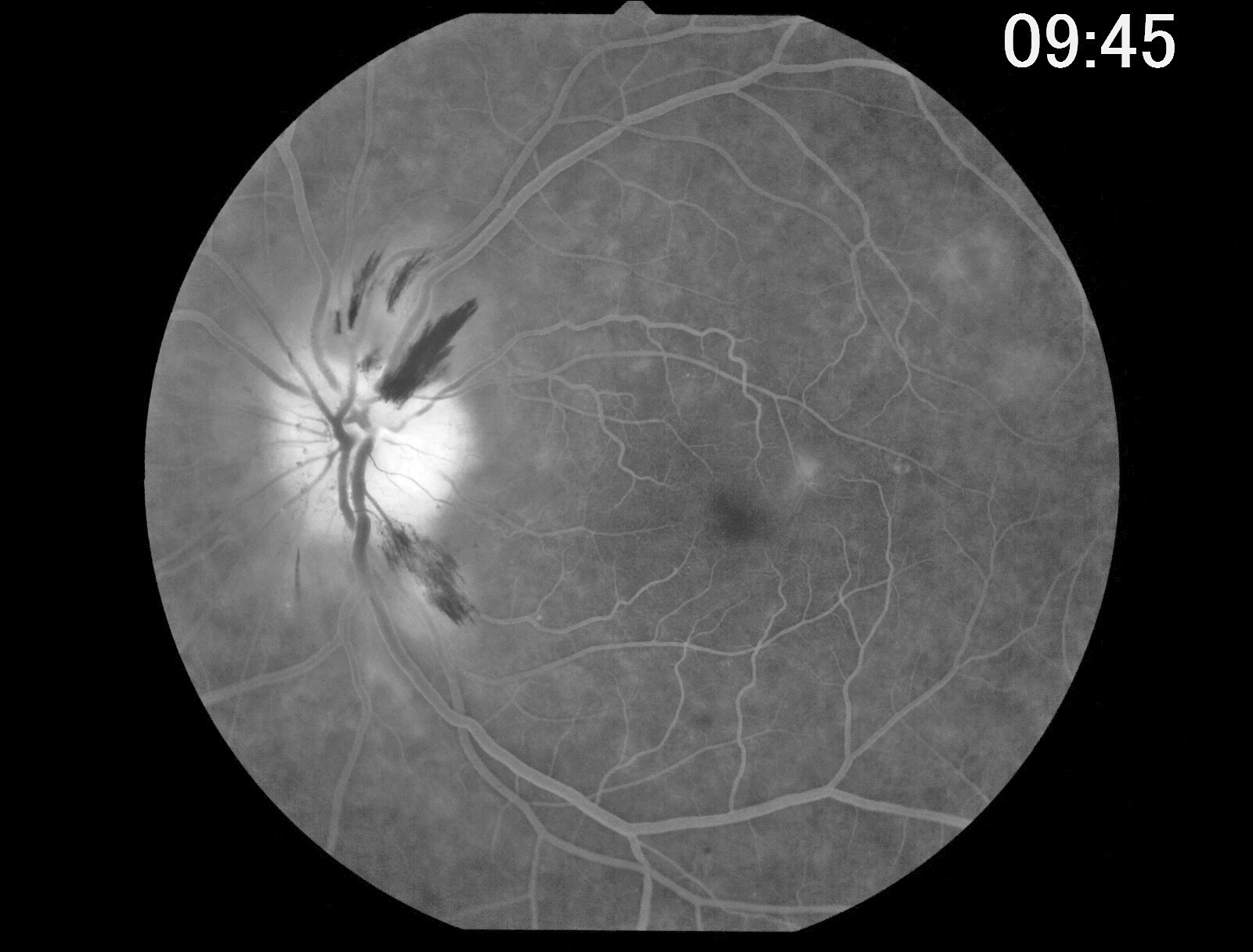
 and florid disc edema OS with retinal vasculitis predominantly involving the veins (image 1). On fluorescein angiography, the retinal veins in the left eye diffusely stained (image 2) with optic nerve leakage in the right eye (image 3). On further review of systems, she had a new skin rash on her right forearm, but was otherwise asymptomatic. Testing revealed elevated angiotensin converting enzyme, lysozyme, and a chest x-ray showing bilateral perihilar fullness. With a working diagnosis of sarcoidosis, she is currently being managed with oral steroids and has been evaluated by both rheumatology and pulmonology. While her retinal vasculitis has responded well to treatment, her vision remains HM three weeks later (image 4). Frosted branch angiitis is a retinal vasculitis that gets its name due to the involved vessels resembling the branches of a tree that are “frosted” with snow. Although these findings may be isolated, they are often considered more of a phenotype that can be found in a multitude of inflammatory conditions, most commonly CMV retinitis. The inflammation is usually very responsive to steroids and the visual prognosis is generally good, although some can develop secondary anterior and posterior segment neovascularization from widespread ischemia. This case can be found on www.retinarocks.org, in the Image Library, Sarcoidosis folder, Sarcoidosis IFH-.")


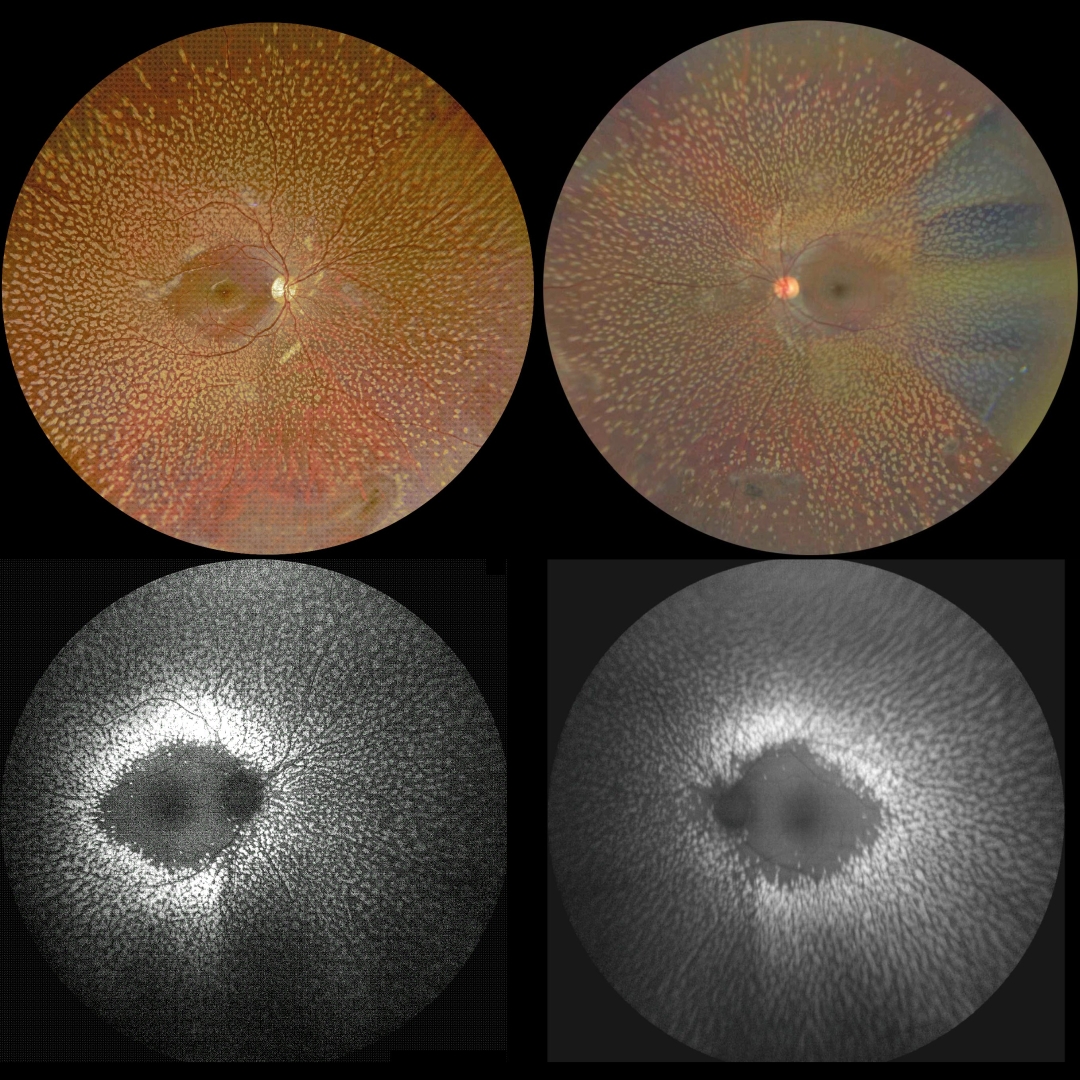
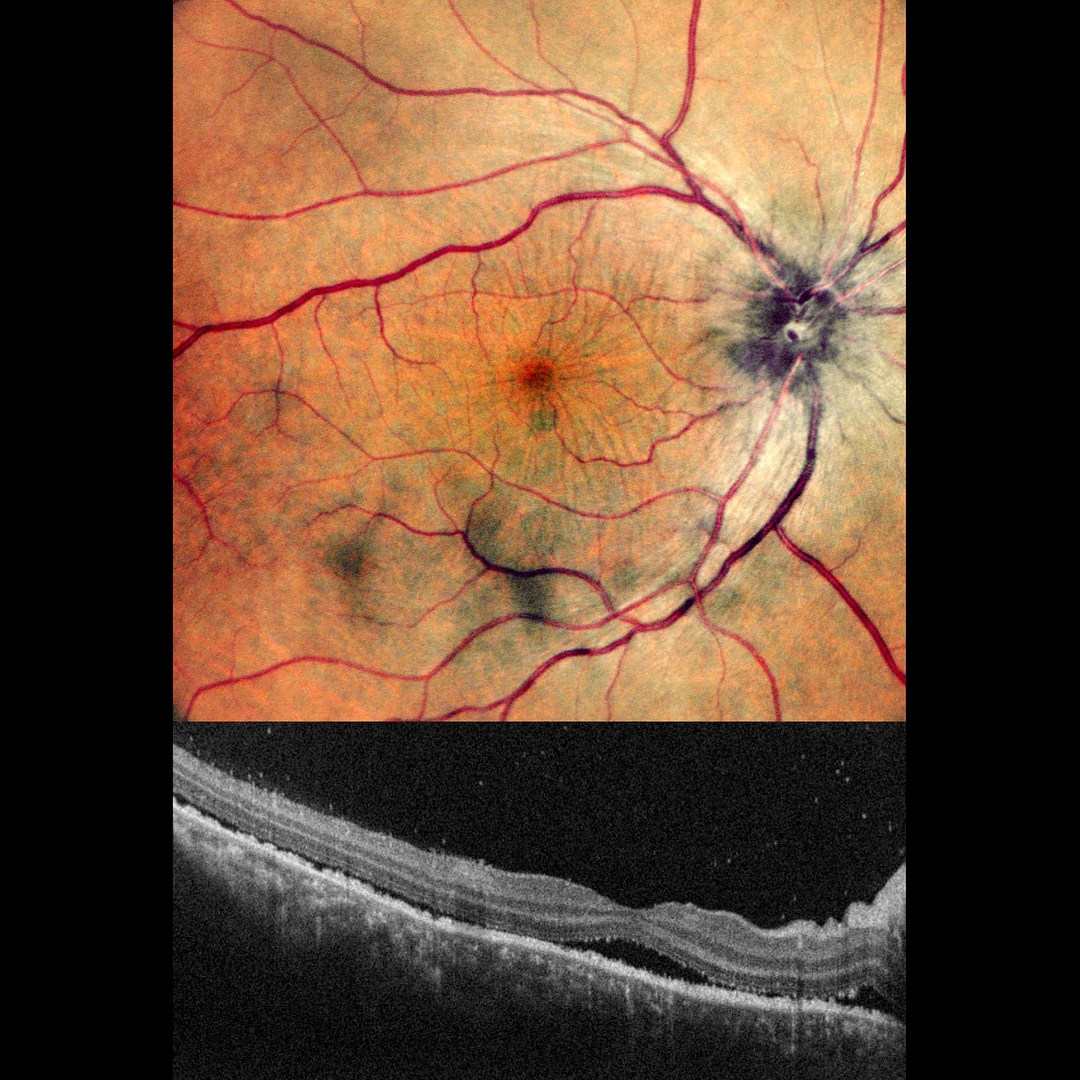
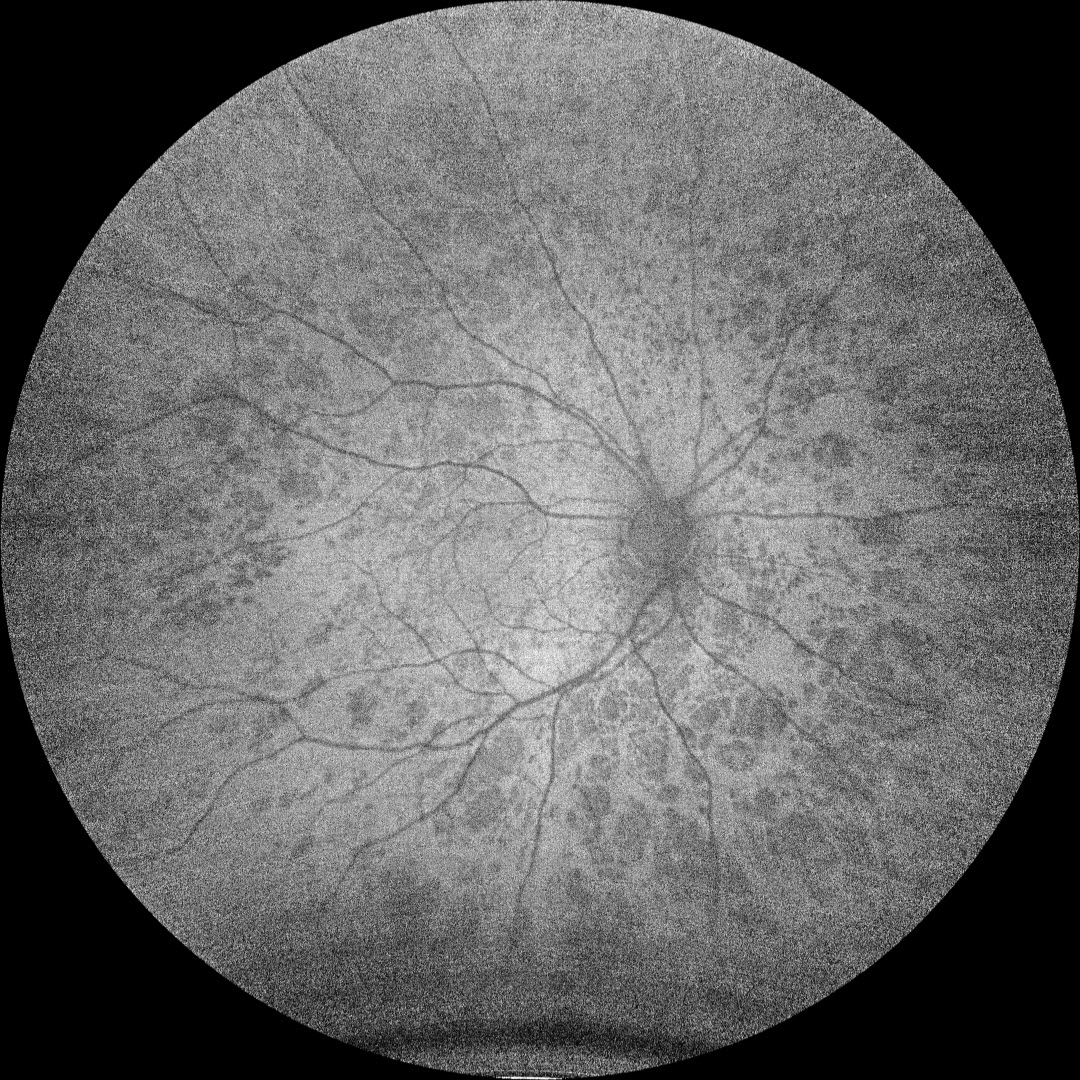
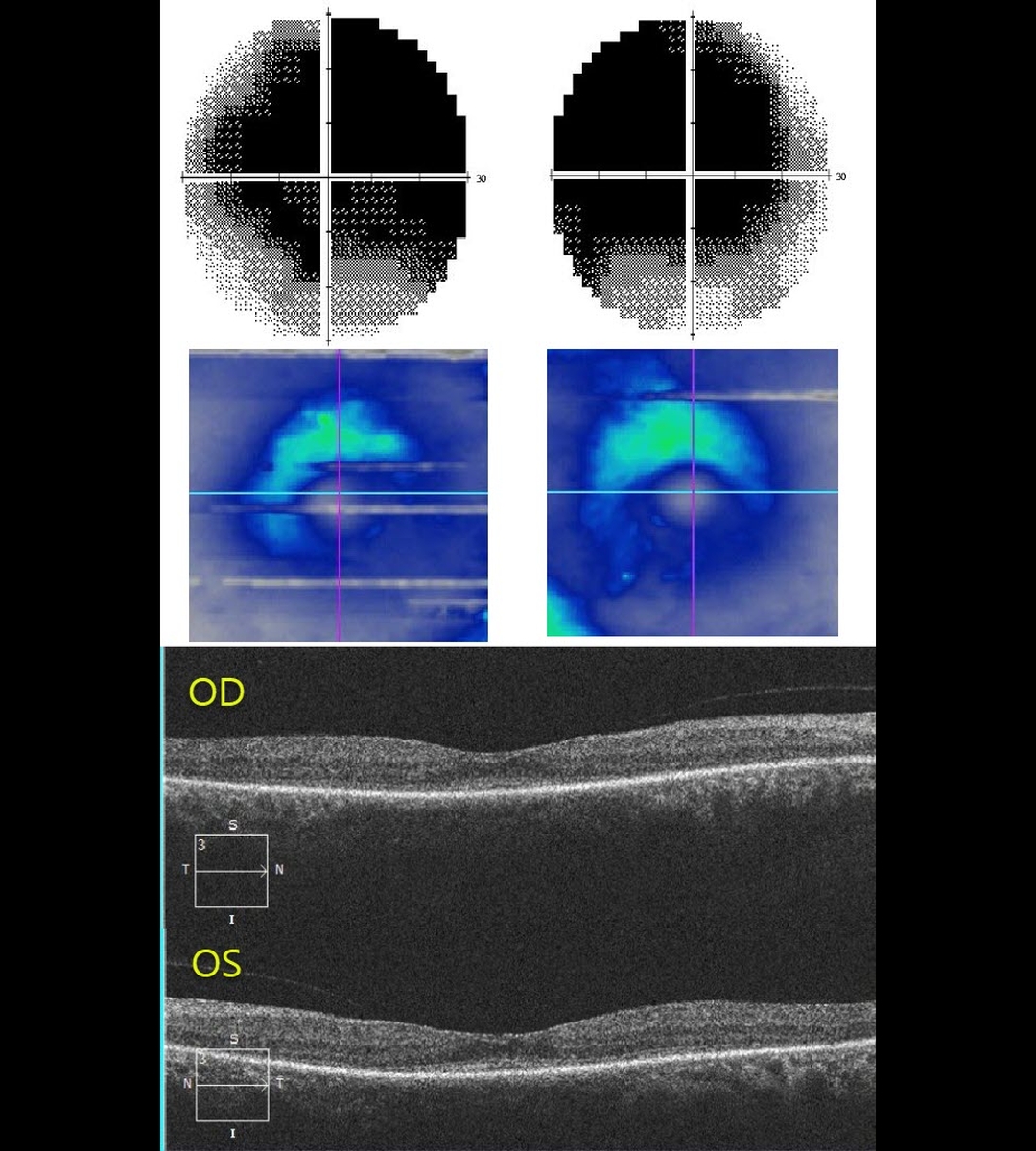
 and fundus autofluorescence (FAF, right) imaging show extremely symmetrical findings (image 1). A gutter of pigment loss extends along the inferotemporal arcades and inferior to the optic nerve into the inferior peripheries where there is more extensive chorioretinal scarring with intraretinal pigment migration. The gutters are classic for subretinal exudation, most commonly central serous chorioretinopathy (Yannuzzi et al, Ophthalmology 1984;91:1554-1572). The intraretinal pigment migration can also be seen following blunt trauma (pseudo-RP). VF testing shows marked diffuse depression (image 2, top). Triton swept-source OCT shows marked retinal thinning (image 2). OCT B-scanning shows outer retinal thinning and a probable thickened choroid bilaterally, possibly supporting the central serous diagnosis. However, the marked symmetry of all these findings made us feel that trauma or central serous were unlikely. Subsequent workup included full field electrophysiology and genetic testing. Dark adapted ERG showed normal amplitudes, but the light adapted and cone flicker were severely reduced. Her genetic testing revealed pathologic mutations in the NPHP1, ABHD12, LRP5 and PDE6A genes. The NPHP1 mutation, coupled with her retinal findings and kidney history confirmed a rare genetic autosomal recessive renal-retinal syndrome known as Senior-Løken Syndrome. This was first described independently in 1961 by Senior et al as juvenile familial nephropathy and tapetoretinal degeneration (AJO 1961;52:625-633) and Løken et al as hereditary renal dysplasia and blindness (Acta Paediatrica 1961;50:177-184). Cystic kidney disorders known as nephronophthisis accompany the retinal findings which are part of the broader category of retinal ciliopathies (Adams et al, Ophth Genetics 2007;28:113-125) including leber congenital amaurosis and some variants of retinitis pigmentosa. Less than 200 cases of Senior-Løken have been reported. This case can be found on www.retinarocks.org, in the Image Library, Retinitis pigmentosa (RP) + Misc Inherited retinal diseases (IRD) folder, RP HSZ-.")
. A vertical OCT B-scan through this lesion (bottom) showed choroidal hyporeflective thickening (red arrow), an overlying subretinal/intraretinal hyperreflective lesion (orange arrow), and superior subretinal fluid (yellow arrow). Laboratory testing was positive for QuantiFERON-TB Gold, and negative for FTA, CBC, ACE. Unfortunately, despite numerous attempts to reach this patient, she was lost to follow up. Tuberculosis (TB) is a systemic disease caused by Mycobacterium tuberculosis, characterized by caseating granuloma formation throughout the body. Although pulmonary involvement is the most common, extrapulmonary sites can include the gastrointestinal, skin, cardiovascular, genitourinary, and central nervous systems including the eyes. Ocular involvement, similar to syphilis, can mimic virtually any type of uveitis including anterior, intermediate, posterior, and panuveitis, retinitis and retinal vasculitis, neuroretinitis, optic neuropathy, and choroidal granuloma (this patient), choroiditis and scleritis. For an excellent review of intraocular tuberculosis, see Bupta et al, Survey Ophthalmology 2007;52:561-587. This case can be found on www.retinarocks.org, in the Image Library, Tuberculosis folder, Tuberculosis DOL-.")
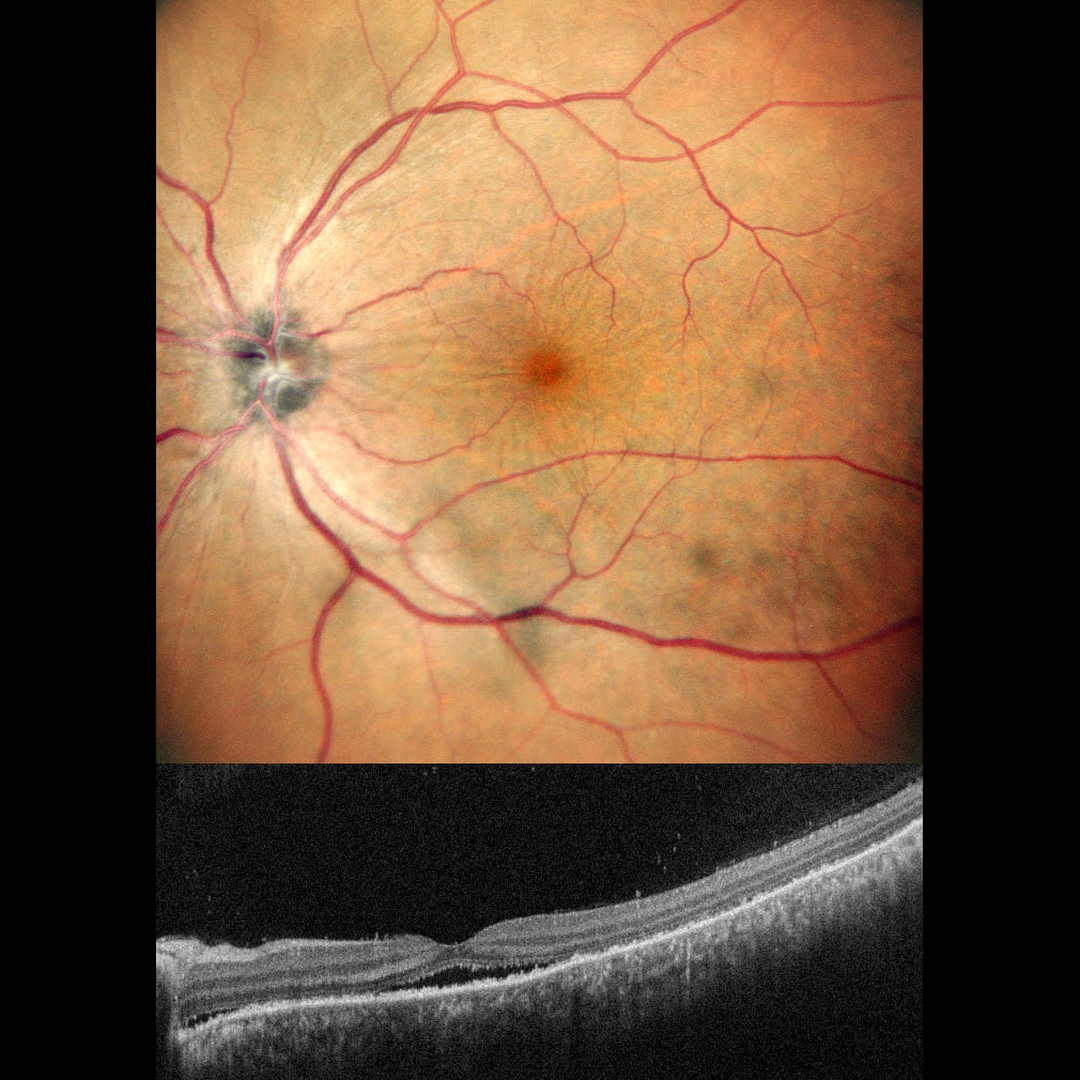
. Vision was 20/25 and there was no afferent pupillary defect (APD). OCT scanning showed some mild cystic fluid in the peripapillary inner outer nuclear layer (image 1, bottom). Fluorescein angiography showed diffuse optic nerve leakage (image 2). Blood pressure was normal. He denied deer tick or cat scratch exposure, and MRI scanning was normal. The funduscopic findings spontaneously normalized within a few months. Diabetic papillopathy, often a diagnosis of exclusion, is most commonly seen in type 2 diabetics. It has a good visual prognosis with observation alone. A small physiologic cup may predispose to this condition (see Regillo et al, Arch Ophthlamol 1995;113:889-895). Unlike ischemic optic neuropathy, vision is usually quite good, there is usually no APD, the nerve swelling is more diffuse than sectorial, and there is no altitudinal field defect. The differential for unilateral acute optic nerve swelling has a wide differential including diabetes, ischemic (anterior ischemic optic neuropathy) and inflammatory (optic neuritis, bartonella, syphilis, sarcoidosis). Papillitis must be differentiated from papilledema, which is bilateral optic nerve swelling caused by elevated intracranial pressure. We have been burned more than once from unilateral nerve edema being the only presenting sign from severe hypertension. Although nerve swelling is usually bilateral in hypertensive retinopathy (see our 4/10/20, 9/7/21, 12/22/20 and 3/9/21 posts), we therefore always check blood pressure in all patients presenting with either uni- or bilateral optic nerve swelling. This case can be found on www.retinarocks.org, in the Image Library, Optic nerve (ON) papillitis folder, ON papillitis SZN-.")
 was successfully treated with initial photodynamic therapy (PDT) (due to the presence of subretinal fluid) followed by transpupillary thermotherapy (TTT) once dry. He developed a secondary branch retinal vein occlusion (BRVO), likely due to thermal damage from the TTT (arrow). BRVO’s are virtually always caused by an artery compressing a vein at a shared arteriovenous crossing. However, rarely, they can occur due to other causes, including inflammation (most commonly sarcoidosis) or secondary to interventions such as TTT. Vision is 20/30 and we continue to follow him closely. Scatter laser will be needed if he develops increasing ischemia with neovascularization from the BRVO. This case can be found on www.retinarocks.org, in the Image Library, Cancer 1 Uveal malignant melanoma (MM), Uveal MM NZG-.")
. The outer plexiform layer (OPL, red arrow) marks the innermost portion of the intact photoreceptors more peripherally. The loss of the photoreceptors is seen as the OPL descends towards the RPE, eventually resulting in fairly complete outer retinal and RPE atrophy (yellow arrow).
Stargardt’s disease is an autosomal recessive disorder caused by a mutation in the ABCA4 gene. The ABCA4 protein is located in the photoreceptor outer segments and is involved in the recycling of 11-cis-retinal. The mutation of this gene causes accumulation of lipofuscin in the RPE, which eventually leads to photoreceptor and RPE degeneration. Other ABCA4 disorders include fundus flavimaculatus and cone-rod dystrophy. This case can be found on www.retinarocks.org, in the Image Library, Stargardt's disease folder, Stargardt's disease HRN-.")

 tears, and retinal dialysis (break at the ora serrata). In general, asymptomatic retinal breaks are observed since they are at low risk for causing a retinal detachment. Symptomatic retinal tears and retinal dialysis are at highest risk for causing a detachment and are virtually always treated. Situs inversus is a congenital abnormality where the retinal vessels exit the optic nerve with a nasal bend prior to heading temporally. Occurring in 1 to 2% of the population, it is sometimes associated with a tilted optic disc. This case can be found on www.retinarocks.org, in the Image Library, Retinal break folder, Retinal break GFI-.")
 was detached throughout the entire macula (arrows), and an inferior layered sub-ILM hemorrhage spared the macular center. Her hemoglobin was later found to be 11. Acute sub-ILM hemorrhage is most common following a Valsalva maneuver or trauma (which our patient denied) but can also happen spontaneously with anemia. These hemorrhages virtually always resolve without sequelae, although the blood can be drained into the inferior vitreous by creating a small opening in the ILM using either a thermal or Nd:YAG laser. Unfortunately, we have no further clinical information on our patient. This case can be found on www.retinarocks.org, in the Image Library, Anemia folder, Anemia DRO-20110203.")
 morning glory folder, ON Morning Glory XLM-20200910.")

 with periodic photodynamic therapy for symptomatic foveal fluid in his left eye, this patient presented with new unilateral diffuse pigmentary deposits (image 1). Fundus autofluorescence (FAF, image 2) shows a dramatic pattern of hyperautofluorescent and hypofluorescent spots scattered throughout the fundus. These findings, although unilateral, look very similar to those in the paraneoplastic condition, bilateral diffuse uveal melanocytic proliferation (BDUMP). Macular OCT scanning shows a diffusely thickened choroid (red line) when compared to the neurosensory retina (yellow line) (note that the choroidal and neurosensory retinal thicknesses are usually comparable). Other OCT findings here include a few large central foveal cysts, outer retinal atrophy (indistinguishable ellipsoid and interdigitation zones), and RPE changes (irregular small RPE elevations and mostly central RPE thinning/loss). The right eye had stable typical PPS findings of a thickened choroid, chorioretinal folds and secondary overlying central pigmentary changes (images 4 and 5). In BDUMP, the thickened choroid and pigmentary changes are secondary to infiltration of benign uveal melanocytes, possibly in response to a primary visceral tumor producing melanocytic growth factors. Our patient has no known prior cancer diagnoses, and recently had a negative CT abdominal scan and chest x-ray. He continues to be followed closely by his internist since BDUMP often precedes the diagnosis of a systemic malignancy by months to years. This case can be found on www.retinarocks.org, in the Image Library, Peripapillary pachychoroid syndrome folder, YOV-.")



 presented with some symptomatic superior field loss. A yellow and red subhyaloid hemorrhage was noted in the inferior macula. The more dependent red blood is hypoautofluorescent and the devitalized, more superior yellow blood is intensely hyperautofluorescent. Devitalized blood includes breakdown products of hemoglobin, including free bases (the heme porphyrin molecule without its iron ion). The free bases absorb blue light and thus appear yellow. The causative neovascularization is likely beneath the blood since angiography shows no leakage. On OCT, the yellow blood is hyperreflective throughout, and the red blood is hyperreflective on its surface and shadows more posteriorly. This case can be found on www.retinarocks.org, in the Image Library, DR (Diabetic retinopathy) 08 PDR folder, DR PDR ILW-.")
 simulates a macular pattern dystrophy due to accumulation of hyperautofluorescent subretinal yellow vitelliform material. The multiple islands of macular atrophy, best seen on fundus autofluorescence, are classic for this disorder. It is caused by an A3243G mutation in mitochondrial DNA and is responsible for up to several percent of people diagnosed with Type 2 diabetes. Check out the full set of images in the Retina Rocks collection, dating back to 2012, to see the progression of the parafoveal macular atrophy. This case can be found on www.retinarocks.org, in the Image Library, Maternally inherited diabetes and deafness (MIDD) folder, MIDD ZXP-.")

 of a patient with prominent disc neovascularization (NVD) from proliferative diabetic retinopathy. This image captures blood vessels from the full thickness retina, including the superficial radial peripapillary capillary network, which is not imaged with traditional fluorescein angiography, Movement artifacts are noted throughout the scan (arrows). Image 2 shows the fundus photograph and image 3 isolates the vitreoretinal interface showing just the NVD. This case can be found on www.retinarocks.org, in the Image Library, DR (Diabetic retinopathy) 08 PDR folder, DR PDR XFI-.")


, have a sunflower appearance showing features of both exudative and tractional cystoid spaces. The macular hole should be hyporeflective centrally. It is hyperreflective in this image due to the OCT software mis-identifying the RPE as being within the mid-retina. This case can be found on www.retinarocks.org, in the Image Library, Macular hole folder, Macular hole IZH-.")
 Rhegmatogenous (RRD) folder, RRD VIR-20191029 thru VIR-.")







 11 TRD & PPV folder, DR TRD NZQ-.")




 08 PDR folder, DM PDR VZH-.")
 pseudoduplication folder, DR PDR HVZ-.")


 Rhegmatogenous folder, RD Rhegmatogenous DLL-.")






 folder, Retinal AVM YRM-.")